Wart Plantar (ICD-10: B07) ⚠️
Plantar Wart (Verruca Plantaris): A Common Viral Neoplasm of the Foot
Overview
Plantar warts, also referred to as verruca plantaris, are benign skin tumors of viral origin that typically develop on the weight-bearing surfaces of the feet. Caused by specific strains of the human papillomavirus (HPV), they are most frequently diagnosed in children and adolescents, affecting up to 10% of this population. These warts are distinct for their deep location, keratinized surface, and frequent resistance to treatment, especially in older individuals.
Plantar warts often appear singly but can also occur in clusters or merge into large mosaic lesions. Due to the pressure from walking, these warts may grow inward rather than outward, making them painful when walking or standing for long periods. This distinguishes them from warts in other locations, which are usually asymptomatic.
Predisposing Factors and HPV Transmission
The underlying cause of plantar warts is infection with HPV, typically low-risk cutaneous types such as HPV 1, 2, 4, or 57. Despite the high global prevalence of HPV (up to 90% of the adult population may be carriers), only a subset of individuals develop visible warts, highlighting the importance of additional predisposing factors for clinical manifestation.
These factors include:
- Immunodeficiency: Including immunosuppressive therapy, chronic diseases, HIV infection;
- Endocrine and metabolic disorders: Diabetes, obesity, hormonal imbalances;
- Chronic skin trauma: Micro-tears from walking barefoot, tight shoes, or excessive physical activity;
- Excessive foot perspiration: Creates a moist environment favorable to HPV survival and entry;
- Contact with contaminated surfaces: Public showers, gyms, swimming pools;
- Poor foot hygiene: Infrequent washing, improper drying, shared footwear or socks;
- Psychophysiological stress: Weakens the immune system and increases viral susceptibility.
Transmission occurs via direct skin contact with viral particles or indirectly via contact with infected surfaces. The virus penetrates the skin through minor abrasions and settles in the basal layer of the epidermis, where it triggers the abnormal proliferation of keratinocytes.
Diagnosis of Plantar Warts
The diagnosis of plantar warts is based on clinical evaluation, considering lesion appearance, location, and patient symptoms. Due to the thick keratin layer and pressure from body weight, plantar warts may resemble calluses or corns.
Additional diagnostic approaches include:
- Dermatoscopy: Enables identification of characteristic vascular patterns and keratin plugs;
- HPV DNA testing: May be used for recurrent or atypical warts to determine viral subtype;
- Histological examination: Performed if malignancy is suspected or to confirm the diagnosis in refractory lesions.
Symptoms and Clinical Features
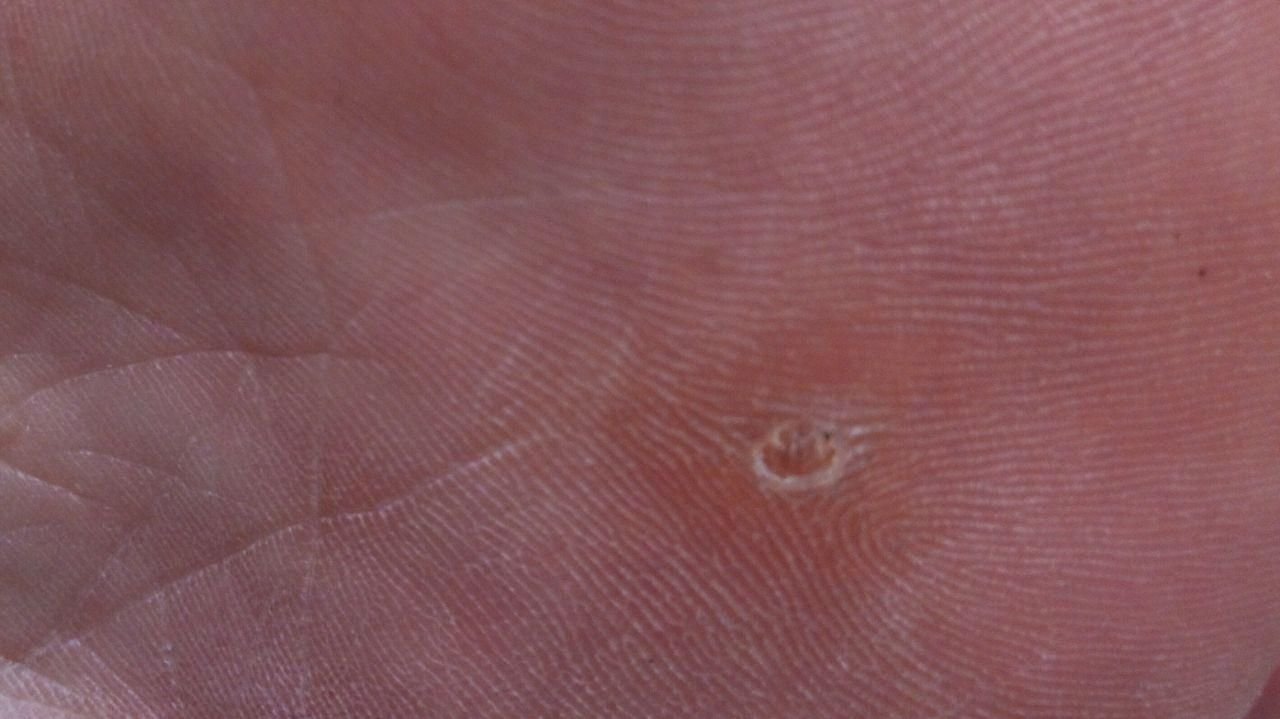
Plantar warts appear as flat or slightly elevated lesions with a rough, thickened surface and often a keratin plug at the center. Their growth is often directed inward due to pressure from standing and walking.
Clinical characteristics include:
- Location: Soles of the feet, especially weight-bearing areas like the heel or forefoot;
- Size: Typically 2–5 mm in diameter; larger lesions may result from confluence of multiple warts;
- Surface: Coarse, with fine papillae or papillary ridges, often with visible thrombosed capillaries;
- Color: Flesh-colored, pale, or grayish, depending on keratin content and age of lesion;
- Margins: Well-defined with a keratinized border separating the lesion from healthy skin;
- Symptoms: Pain or tenderness when walking, pressure sensitivity, and possible tingling or discomfort.
Dermatoscopic Description
Dermatoscopy is an invaluable tool for differentiating plantar warts from other keratotic lesions. Classic findings include:
- “Frogspawn” pattern: Clustered papillae each surrounded by a white keratin ring and containing a central red or black dot (capillary loop or thrombosed vessel);
- Yellowish structureless zones: Caused by hyperkeratosis from weight-bearing pressure;
- Pale corolla at the edge: Marks the transition to healthy skin;
- Linear ridges or grooves: Occasionally seen due to the compression of dermal structures by body weight.
These features help differentiate plantar warts from corns, calluses, seborrheic keratoses, and pigmented lesions.
Differential Diagnosis
Plantar warts must be differentiated from other skin lesions on the soles of the feet, as their appearance can mimic several common and uncommon conditions. Important differential diagnoses include:
- Corn (clavus): Central core surrounded by keratin; lacks vascular puncta and is usually less painful on side pressure;
- Callus: Diffuse thickening of the stratum corneum without central vessels or pain on vertical pressure;
- Flat wart: Smooth surface, smaller size, often found on the face or hands;
- Common wart: More raised, rougher surface, typically found on hands or periungual areas;
- Dermatofibroma: Firm, hyperpigmented lesion with a “dimple sign” when squeezed laterally;
- Pigmented nevus: Stable, symmetrical pigmented lesion; may need biopsy if change is observed;
- Molluscum contagiosum: Central umbilicated papules with a pearly appearance, more common in children;
- Amelanotic melanoma: Rare, but must be ruled out in rapidly changing or atypical plantar lesions.
Risks and Clinical Implications
Plantar warts are considered non-cancerous and carry no inherent oncogenic risk under normal conditions. However, certain clinical scenarios may warrant closer observation, particularly when:
- The lesion changes rapidly in shape, color, or texture;
- Pain worsens or bleeding occurs without trauma;
- The wart recurs quickly after removal or spreads to nearby areas;
- The patient has a known immunosuppressive condition.
Additional concerns include:
- Physical discomfort: Pain during ambulation or exercise can reduce mobility and affect quality of life;
- Injury and bleeding: Constant pressure increases the risk of skin breakdown and secondary bacterial infection;
- Psychological stress: Visibility, especially in multiple lesions, may cause self-consciousness or embarrassment;
- Immune dysfunction: Multiple or recalcitrant lesions may reflect reduced immune control over HPV infection.
Tactics: Monitoring and Clinical Management
In cases where plantar warts are asymptomatic and do not interfere with walking or daily activities, regular monitoring and patient education may be sufficient. Observation should be performed at least once per year or more frequently if changes occur.
Patients should promptly consult a dermatologist if:
- Lesions become painful, ulcerated, or increase in number;
- There is trauma, bleeding, or recurrent infection in the wart area;
- They are immunocompromised or have a history of skin malignancy;
- The wart causes gait disturbances, occupational difficulty, or psychological distress.
In such cases, the dermatologist will determine whether to proceed with removal or implement ongoing dynamic observation. For patients with multiple lesions or recurring warts, photographic tracking and lesion mapping are helpful tools for consistent follow-up.
Treatment of Plantar Warts
The choice of treatment depends on lesion size, number, location, patient age, and pain intensity. Less invasive treatments are generally preferred for children or those with few warts.
- Laser therapy: Effective for resistant lesions, with minimal scarring;
- Cryotherapy: Freezing the wart with liquid nitrogen; may require several sessions;
- Radio wave surgery: Suitable for larger or clustered lesions;
- Electrocoagulation: Thermal cautery to destroy wart tissue, used in combination with curettage;
- Topical agents: Salicylic acid, imiquimod, or 5-FU preparations can soften keratin and stimulate immune response (requires prolonged application);
- Surgical excision: Reserved for diagnostic uncertainty or cases resistant to conservative methods. Histology is recommended for all excised lesions.
Self-treatment is discouraged due to risk of incomplete removal, infection, bleeding, and difficulty distinguishing benign from malignant growths.
Prevention of Plantar Warts
Effective prevention of plantar warts involves protecting the skin, controlling HPV exposure, and maintaining immune health. Key measures include:
- Wearing protective footwear: Especially in public showers, locker rooms, and pool areas;
- Practicing foot hygiene: Keep feet clean and dry, and change socks regularly;
- Disinfecting personal items: Do not share towels, shoes, or nail clippers;
- Maintaining strong immunity: Through healthy diet, stress reduction, sleep, and physical activity;
- Avoiding trauma: Choose properly fitting shoes and use insoles if needed;
- Routine dermatological screening: Especially in individuals with multiple lesions or a history of viral warts;
- UV protection: Avoid direct trauma and radiation to the skin, especially during summer months.
With prompt attention, safe treatment methods, and preventive care, plantar warts can be effectively controlled—minimizing recurrence, discomfort, and viral transmission risk.