Trichomycosis (ICD-10: B35) 🚨
Trichomycosis: Fungal Infections of the Scalp and Facial Hair
Overview
Trichomycosis is a general term used to describe fungal infections of the hair and hair follicles, primarily affecting the scalp and beard regions. These infections are caused by dermatophytes—filamentous fungi that have a particular affinity for keratinized tissues. The main genera responsible for trichomycosis include Microsporum and Trichophyton. Depending on the site of infection, trichomycosis is classified into:
- Tinea capitis: Dermatophytosis of the scalp and hair shafts;
- Tinea barbae: Fungal infection involving the beard or mustache area in adult males.
Trichomycosis is a contagious condition, and outbreaks may occur in schools, families, or close-contact settings. It is considered a quarantine infection in some regions due to its epidemic potential, especially among children. Prompt diagnosis and treatment are important to prevent scarring, hair loss, and further spread.
Patterns of Fungal Invasion
The clinical presentation of trichomycosis depends on the type of dermatophyte and the pattern of hair shaft invasion. Two main invasion patterns are identified:
- Ectothrix invasion: Fungal spores (arthroconidia) develop outside the hair shaft; typical of Microsporum species;
- Endothrix invasion: Spores form within the hair shaft; more often seen in Trichophyton infections.
Clinical Forms of Tinea Capitis
1. Non-Inflammatory (Superficial) Type
This form is commonly caused by anthropophilic fungi such as Trichophyton tonsurans (endothrix) and Microsporum canis or M. ferrugineum (ectothrix).
- Lesions: Round or oval scaly patches with mild redness or none at all; flaking and hair breakage are frequent;
- Hair: Often broken at the scalp surface, creating bald patches with short hair stubs (“black dot” appearance);
- Location: Primarily the frontal and temporal scalp;
- Wood’s lamp: Hair infected with Microsporum fluoresces greenish under UV light;
- Appearance: In seborrheic type, resembles dandruff or dry seborrhea.
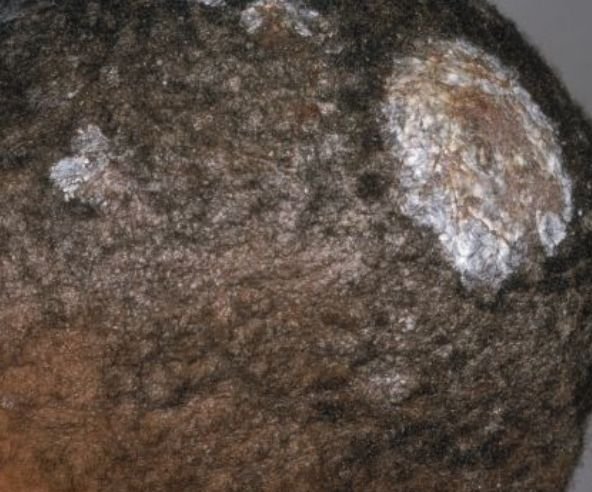
2. Inflammatory Type (Kerion)
Triggered by zoophilic species like Trichophyton gypseum or Microsporum canis. This variant leads to a deep, painful inflammatory lesion.
- Lesions: 1–3 swollen, pustular plaques with intense erythema and purulence;
- Hair: Loosens easily and may fall out or be removed without resistance;
- Risk: May lead to cicatricial (scarring) alopecia if not treated promptly;
- Symptoms: Pain, edema, regional lymphadenopathy, and systemic malaise may be present.
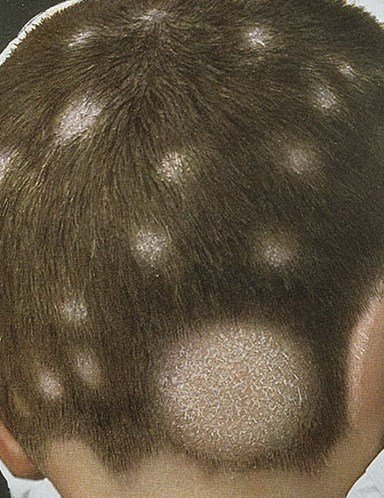
3. “Black Dot” Tinea Capitis
This is the least inflammatory form of scalp ringworm and is caused by Trichophyton tonsurans. The hallmark feature is the presence of short, broken hairs at follicular openings which appear as black dots on close examination.
- Lesions: Multiple round or irregular patches, covered with fine scaling;
- Hair: Broken off at or below scalp level, producing black dot pattern;
- Complications: Risk of chronic infection and atrophic alopecia.
Clinical Forms of Tinea Barbae
Tinea barbae affects adult males in the beard and mustache area and is most commonly caused by zoophilic fungi such as Trichophyton mentagrophytes and T. verrucosum.
1. Inflammatory Type (Parasitic Sycosis)
- Symptoms: Painful, nodular, and pustular lesions resembling kerion, with purulent discharge from follicular openings;
- Hair: Easily extracted with purulent material at the base.
2. Superficial Type
- Lesions: Mild follicular inflammation, erythema, and scaling that resemble bacterial folliculitis;
- Inflammation: Less severe than the kerion-type presentation.
3. Annular Type
- Appearance: Ring-shaped patches with elevated, scaling borders containing vesicles or crusts;
- Central area: Tends to clear partially, forming a classic tinea ring pattern similar to tinea corporis.
Diagnosis of Trichomycosis
Accurate diagnosis of trichomycosis is critical for effective treatment and infection control. Diagnostic steps include:
- Wood’s lamp examination: Useful for detecting Microsporum species, which fluoresce under UV light;
- Microscopy: Direct KOH examination of plucked hairs or skin scales to detect fungal hyphae or spores;
- Cultural examination: Inoculation on Sabouraud agar allows for fungal identification and differentiation;
- PCR testing: Highly specific molecular technique used to identify fungal DNA in clinical specimens;
- Epidemiological investigation: Important in the context of outbreaks or school-based transmission.
Differential Diagnosis
Trichomycosis can mimic various dermatologic and systemic conditions, making differential diagnosis essential to avoid mismanagement. Important conditions to distinguish from include:
- Alopecia areata: Sudden onset of patchy hair loss with smooth skin, no scaling or inflammation;
- Discoid lupus erythematosus: Erythematous, scarring plaques with follicular plugging and atrophy;
- Psoriasis and seborrheic dermatitis: May present with scaling on the scalp but lack hair breakage or inflammation;
- Pseudopelade of Brocq: Slowly progressive scarring alopecia with smooth, ivory-colored patches;
- Bacterial sycosis (folliculitis barbae): Painful pustules limited to beard area but caused by bacterial infection;
- Secondary syphilis (impetiginous syphilid): Must be ruled out in the presence of scaling and alopecia, especially in high-risk populations.
Treatment of Trichomycosis
Management of trichomycosis involves both systemic antifungal therapy and adjunctive local treatment. Treatment should always be guided by fungal culture and species identification when possible.
Systemic Antifungal Agents:
- Griseofulvin: Traditionally the first-line oral antifungal for tinea capitis and barbae; well-tolerated and suitable for pediatric use (available as suspension);
- Terbinafine: Fungicidal against dermatophytes; used in both children and adults;
- Itraconazole: Broader-spectrum antifungal effective in resistant or recurrent cases.
Systemic treatment is typically prescribed for 6–12 weeks depending on the clinical response, type of fungus, and extent of infection.
Topical Therapy:
Used as adjunctive therapy or primary treatment in very mild, localized cases. Options include:
- Topical antifungals: Miconazole, clotrimazole, terbinafine, or ciclopirox-based creams or pharmacy-compounded agents;
- Iodine-based solutions (2–5%): For daily application on lesions;
- Pharmacy-prepared lotions: Containing salicylic acid, quinosol, dimexide for drying, keratolytic, and antiseptic effects.
Supportive Care and Hygiene During Treatment
Effective treatment requires not only medication but also proper hygiene and behavior modifications to reduce reinfection and transmission:
- Hair care: Shave or clip affected hair weekly during active infection to reduce fungal load;
- Washing routine: Wash hair and scalp 2–3 times per week with warm water and antifungal shampoo;
- Barrier protection: Use gauze or cotton head coverings to prevent spread; discard or sterilize daily;
- Avoid sharing personal items: Towels, combs, hats, razors should not be shared;
- Social hygiene: Limit close contact with others, particularly children, until lesions heal.
Prevention of Trichomycosis
Prevention of recurrence and transmission involves a combination of public health education and personal care:
- Prompt treatment: Seek early medical attention for suspicious lesions of the scalp or beard area;
- Screening contacts: Family members or classmates of infected individuals should be examined for signs of infection;
- Sanitization: Disinfect combs, brushes, and barber tools after each use;
- Pet care: Since zoophilic fungi are often transmitted by animals, inspect household pets and consult a veterinarian if needed;
- Strengthen immunity: Address underlying health conditions, maintain nutrition, and reduce stress;
- Avoid trauma: Prevent scratching and damage to the scalp or beard area that facilitates fungal entry.
Conclusion
Trichomycosis represents a group of infectious dermatophytoses with diverse clinical manifestations depending on the fungal species and host immunity. Early recognition, laboratory confirmation, and appropriate treatment are essential to prevent complications such as scarring alopecia or widespread outbreaks.
With a combination of systemic antifungal therapy, topical agents, personal hygiene, and contact precautions, most cases can be treated successfully. Continued awareness and patient education are key in reducing recurrence and community transmission of fungal hair infections.