Dysplastic Nevus (ICD-10: D22) ⚠️
Dysplastic Nevus (Atypical Nevus, Melanoma-Dangerous Nevus, Clark’s Nevus)
Dysplastic Nevus (also known as atypical nevus, melanoma-dangerous nevus, or Clark’s nevus) is a pigmented melanocytic lesion. Individual dysplastic nevi rarely transform, but patients with multiple atypical nevi have an increased overall melanoma risk and need regular skin surveillance. Dysplastic nevi can appear at any age, though the likelihood increases with age. These lesions tend to be multiple, which is especially common in individuals with multiple congenital nevi, and after excessive exposure to solar or artificial ultraviolet (UV) light. Dysplastic nevi occur with equal frequency in both men and women.
Predisposing Factors
The exact cause of dysplastic nevi is not fully understood. However, several predisposing factors have been identified, which may increase the likelihood of developing these skin neoplasms. These factors can make the skin more susceptible to the formation of dysplastic nevi:
- Genetic Factors (Heredity): It has been found that the appearance of dysplastic nevi can be inherited in an autosomal dominant manner, a condition known as dysplastic nevus syndrome. However, many people develop dysplastic nevi without any family history.
- Ultraviolet Radiation: Exposure to solar or artificial UV radiation accelerates the reproduction of nevus cells (melanocytes) and leads to excessive melanin production, which is observed in the nevus. UV radiation also increases the risk of malignant transformation of these nevi.
- Hormonal Changes: Hormonal fluctuations, especially during puberty or pregnancy, can affect the appearance of new nevi and the growth of existing ones.
- Ionizing Radiation and Skin Injuries: Chronic skin injuries or exposure to ionizing radiation can provoke the appearance or growth of dysplastic nevi.
Diagnostics
The diagnosis of dysplastic nevi is based on clinical examination, which includes a visual inspection of the lesion and dermatoscopy to assess its structure and characteristics. If there is suspicion of malignant growth or if the lesion shows atypical features, a biopsy may be performed to confirm the diagnosis and rule out melanoma.
Symptoms
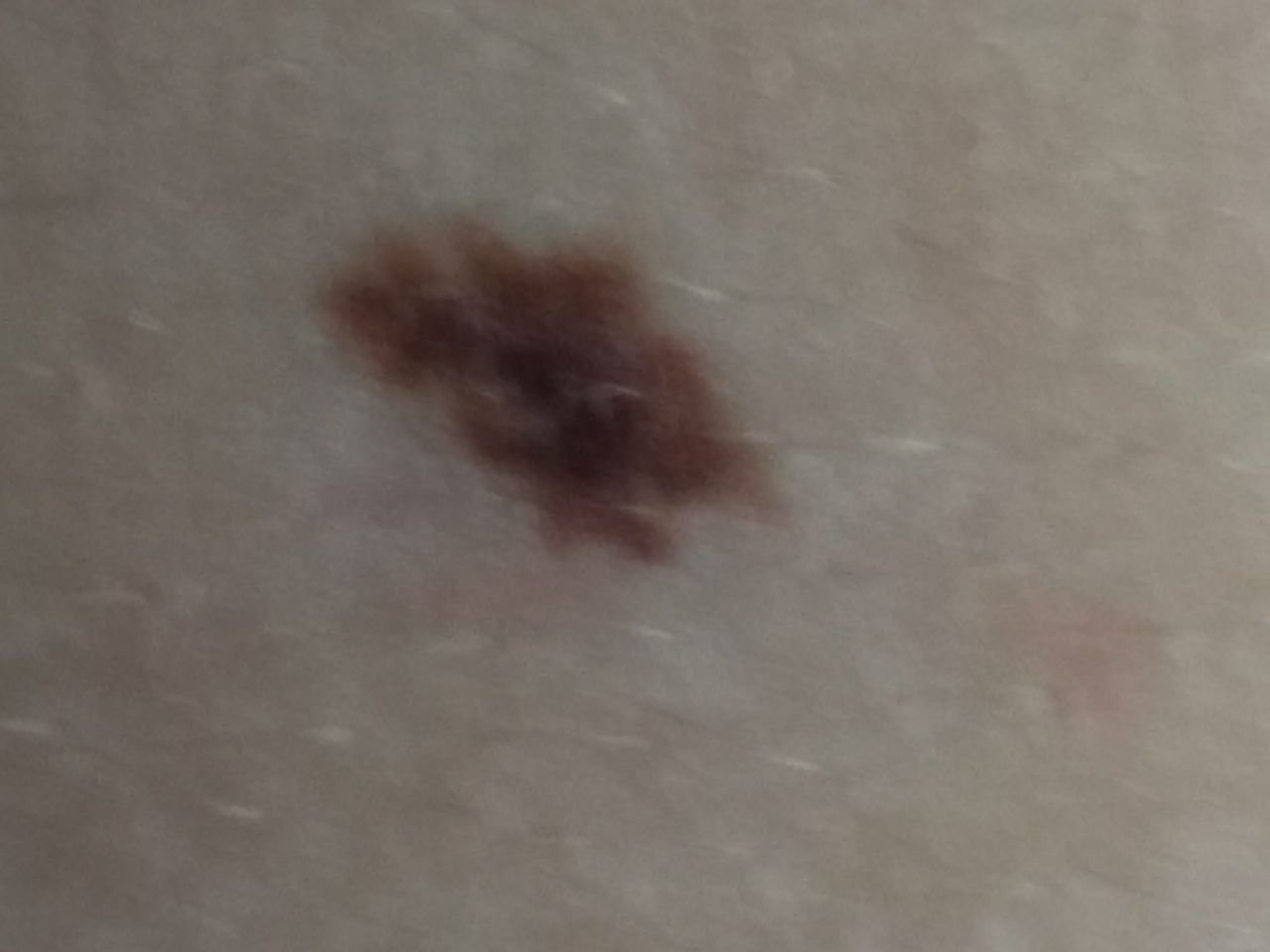
Upon visual inspection, dysplastic nevi present as a spot or slightly elevated nodule. The lesion can be symmetrical (oval, round, or elongated), or irregular in shape. The surface of the nevus may be similar to the texture of normal skin, smooth, or slightly tuberous. In some cases, the nevus may have a rough texture or show peeling.
The borders of dysplastic nevi are usually irregular, with uneven edges that can be considered an unfavorable sign. The color of the nevus can vary widely, ranging from light brown to dark brown, and may also include shades of red, pink, and even blue. The pigment distribution is often heterogeneous, with a gradual decrease in color intensity from the center to the periphery, or different shades of the same color throughout the lesion. In some cases, the nevus may have polychromatic colors, meaning it can contain several colors or their variations.
Hair growth is usually absent in the area of dysplastic nevi, but a sparse hair growth may occasionally be seen at the periphery of the lesion.
The size of a dysplastic nevus usually ranges from 10-15 mm in diameter, although larger lesions can occur. Rapid growth of the nevus is a red flag and can be a sign of potential transformation into melanoma.
On palpation, dysplastic nevi feel slightly denser than normal skin, and there are usually no subjective sensations unless the lesion has been traumatized or exposed to ultraviolet light, in which case mild itching may occur.
Dysplastic nevi can appear anywhere on the body, with no specific location, although they are often found on sun-exposed areas of the skin.
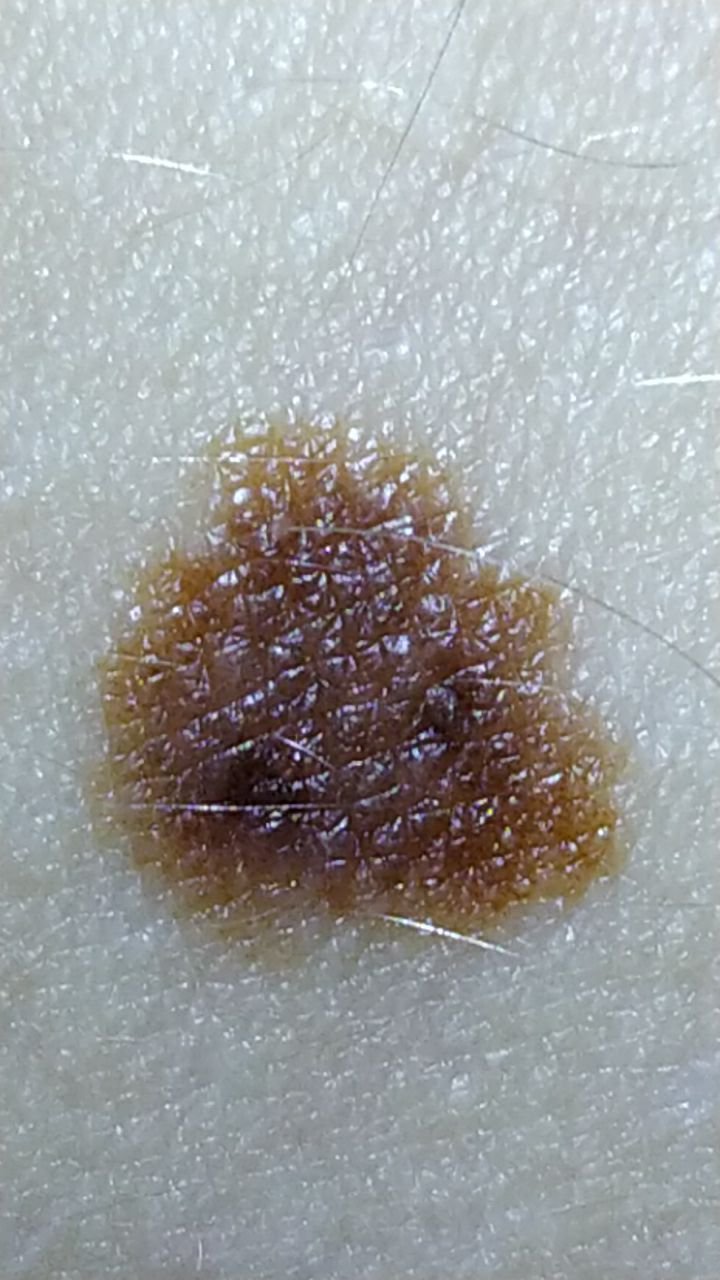
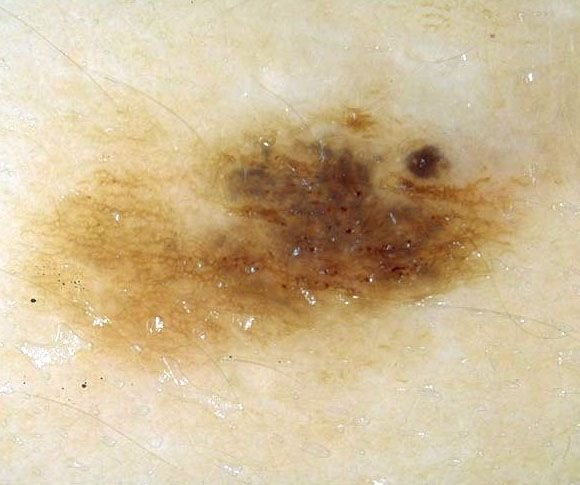
Dermatoscopic Description
Dermatoscopic examination of dysplastic nevi typically reveals the following features:
- Alternating Light and Dark Pigment Network: A pattern of alternating light and dark-colored areas of the pigment network, indicative of an atypical pigment network.
- Irregular Inclusions: Irregular spots and globules are seen against the background of the pigment network, which are a hallmark of dysplastic nevi.
- Globules: These are pigment-filled structures of various sizes and shapes, often visible within the lesion.
- Asymmetry: The color, structure, and shape of the nevus are often asymmetrical, a sign that the lesion may be atypical.
- Uneven Borders: The edges of dysplastic nevi tend to be uneven and irregular.
- Peripheral Radial Radiance: The presence of radial rays extending from the center of the lesion.
- Polychrome (Multiple Colors): Dysplastic nevi often show three or more distinct colors within the lesion.
- Hypopigmentation Zones: Areas with decreased pigment, and sometimes structureless zones, may be visible within the lesion.
- Regression Structures: Signs of regression or involution, which may present as pale areas or incomplete pigmentation.
Differential Diagnosis
It is important to differentiate dysplastic nevi from other pigmented skin lesions, including:
- Post-inflammatory hyperpigmentation
- Congenital dermal melanocytosis
- Pigmented nevus (simple or papillomatous)
- Hemangioma
- Blue nevus
- Spitz nevus
- Basal cell carcinoma
- Melanoma
Risks
Individual dysplastic nevi have a low absolute risk of transformation into melanoma, though UV exposure and chronic trauma are associated with increased risk. Patients with multiple atypical nevi have an increased overall melanoma risk. Dysplastic nevi are melanocytic lesions; the main clinical concern is progression to melanoma in patients with multiple atypical nevi, not transformation into squamous cell carcinoma.
It is essential to monitor dysplastic nevi closely because patients with multiple nevi may have an increased risk of developing other malignant skin lesions, either on the unchanged skin or near the existing nevus. This complicates the timely detection of skin cancer and the differential diagnosis of melanoma.
Tactics
Dysplastic nevi are often difficult to visually differentiate from melanoma in situ (the earliest stage of melanoma). As a result, these lesions are typically removed for histological examination to confirm their benign nature. Dynamic observation may be appropriate for lesions that do not show signs of activity over time, but this should only be done under the supervision of an oncologist. The specialist will determine whether continued monitoring or removal is necessary based on the characteristics of the nevus.
Nevi that are subject to chronic trauma from clothing, jewelry, or professional activities should be removed to prevent further irritation. Dynamic monitoring involves regular photographic documentation of the lesion to track even minor changes in appearance.
Patients with multiple dysplastic nevi should undergo periodic dermatological evaluations, ideally before and after the summer months (to assess the impact of sun exposure). Keeping a map of skin neoplasms can simplify monitoring and help identify new or altered lesions.
Treatment
The treatment of dysplastic nevi typically involves surgical excision using a classic scalpel or a radiofrequency scalpel. After removal, the excised tissue is examined histologically to confirm that the lesion is benign.
Destructive methods, such as laser removal or cryodestruction, are generally avoided for clinically suspicious dysplastic nevi because they do not allow histological evaluation; complete excision with histology is preferred when removal is indicated.
Prevention
Preventing the appearance of dysplastic nevi and minimizing their risk of malignancy involves careful attention to skin care and sun protection:
- Avoiding excessive ultraviolet radiation, including tanning beds and prolonged sun exposure.
- Applying protective creams and wearing appropriate clothing during periods of intense sun exposure.
- Minimizing chronic skin trauma, especially in areas where nevi are present.
- Limiting exposure to ionizing radiation and environmental hazards.
- Maintaining good personal hygiene and staying vigilant for changes in existing nevi.
Regular skin checks, timely consultation with healthcare professionals if any changes occur, and removal of potentially dangerous lesions are crucial for maintaining skin health and preventing complications.