Acne pustular is a chronic inflammatory skin disorder that predominantly affects the sebaceous glands and hair follicles. It is characterized by the development of a wide range of dermatological elements, including comedones (blackheads and whiteheads), papules, pustules, and occasionally nodules or cysts. The most commonly affected areas are the face—particularly the forehead, cheeks, and chin—as well as the upper back, chest, and shoulders, where sebaceous gland activity is most pronounced.
This specific form of acne is distinguished by the dominance of inflammatory lesions—primarily papules and pustules—superimposed on a background of comedonal activity. While comedones may still be present, it is the red, inflamed bumps (papules) and pus-filled lesions (pustules) that define the clinical appearance and progression of pustular acne.
The onset of acne pustular is most frequently observed during adolescence, typically beginning between the ages of 11 and 13. While girls may show earlier signs of breakouts, boys tend to develop more severe and persistent forms of acne. In males, the initial presentation often occurs later—around 18 to 20 years of age—but the intensity and spread are generally greater due to hormonal activity.
Acne pustular affects an estimated 80% of the population at some point in their lives, making it one of the most widespread dermatological issues worldwide. Despite this prevalence, many individuals perceive acne as a purely cosmetic concern and do not seek medical treatment. This delay or neglect can worsen outcomes, leading to complications such as scarring, persistent pigmentation changes, and psychological distress.
The condition is rooted in two primary physiological disturbances: overproduction of sebum by the sebaceous glands, and obstruction of the glandular ducts by dead skin cells and keratin. These two factors contribute to the formation of comedones. Once these clogged follicles become colonized by skin-residing bacteria such as Cutibacterium acnes, a local immune response is triggered, resulting in inflammation and the formation of pustular lesions.
Acne pustular does not stem from a single identifiable cause. Rather, it is a multifactorial disease influenced by a complex interplay of genetic, hormonal, environmental, and behavioral elements. Understanding these risk factors is essential for both prevention and effective long-term management.
The diagnosis of acne pustular is primarily clinical, based on a detailed patient history and a visual examination of the skin. During the consultation, the dermatologist gathers information about the onset, progression, triggers, lifestyle factors, and any previous treatments the patient may have tried. This information helps to determine the type and severity of the acne, as well as to identify potential contributing factors.
During physical examination, the clinician assesses the presence, type, and distribution of lesions—whether comedones, papules, pustules, or nodules. In cases where the clinical picture is not fully clear—such as when lesions are minimal or atypical—dermatoscopy can be used for further clarification. This tool magnifies skin structures and allows for better visualization of patterns, aiding in differential diagnosis.
A thorough assessment is crucial not only for proper classification of acne severity (mild, moderate, severe) but also to rule out other skin conditions that may resemble acne. Accurate diagnosis forms the basis for personalized and effective treatment planning.
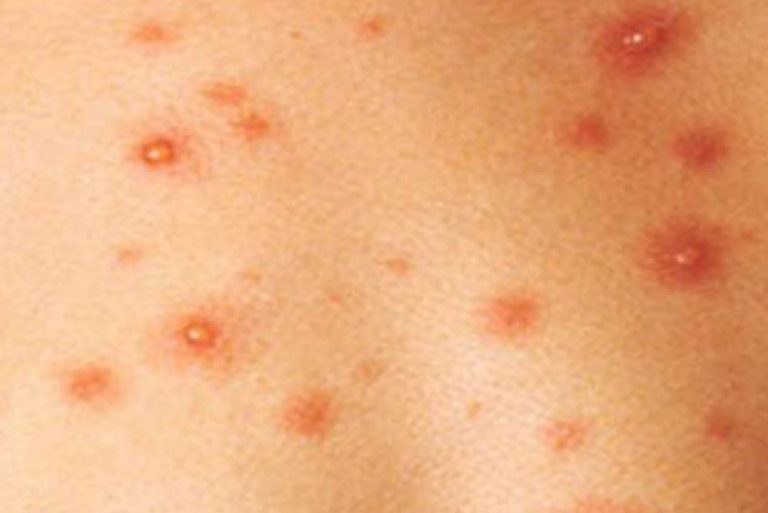
Acne pustular is identified by a combination of non-inflammatory and inflammatory lesions, with papules and pustules being the dominant features. The following elements are typically present:
The preferred areas for pustular acne include the face (forehead, cheeks, chin), the upper back (particularly the scapular region), the chest, and the shoulder girdle. Acne in other body areas is uncommon and typically indicates another dermatologic or systemic issue.
Accurate diagnosis requires ruling out several other dermatologic conditions that can present with similar signs. Conditions to differentiate from include:
Though acne pustular is not life-threatening, it serves as a visible marker of internal processes—some of which may be hormonal, metabolic, or immunological. Neglecting the skin’s condition may result in overlooking deeper, more systemic imbalances.
Moreover, acne pustular has a profound impact on a person’s psychological well-being. Adolescents and adults with moderate to severe acne often suffer from social withdrawal, low self-esteem, and even anxiety or depression. Scarring and hyperpigmentation further compound these challenges.
If left untreated, severe or repeated pustular lesions may rupture, become secondarily infected, and even lead to localized skin abscesses. Therefore, timely intervention is not only about aesthetics—it is about preserving skin integrity and overall health.
At the first signs of persistent or worsening pustular acne, it is critical to consult a dermatologist. Early evaluation helps prevent scarring and identify potential underlying triggers.
Patients should seek medical help when:
Ongoing monitoring and skin care adjustments are necessary throughout the course of the disease. Life transitions—diet changes, climate shifts, new cosmetics, or hormonal treatments—can all trigger flare-ups and should be discussed with a medical provider.
Treating acne pustular requires a comprehensive strategy tailored to the individual. Treatment modalities include:
Patients must avoid interrupting their treatment or using unapproved topical agents. Acne treatment requires time, discipline, and often several months to yield results. Open dialogue with a healthcare provider allows for treatment adjustment and realistic expectations.
While not all cases of acne pustular can be prevented, proactive measures can reduce the likelihood and severity of flare-ups. Key recommendations include:
By combining clinical care, proper skin maintenance, and lifestyle awareness, most cases of acne pustular can be effectively controlled—helping patients regain confidence and maintain long-term skin health.