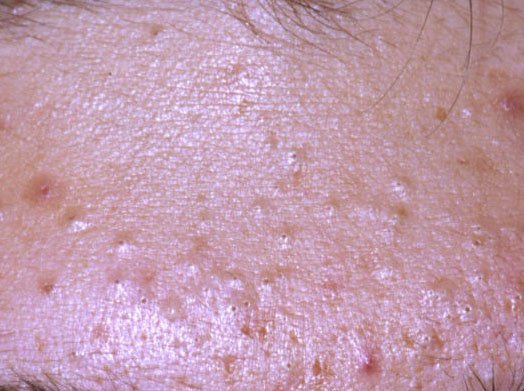
Acne vulgaris is a widespread chronic inflammatory skin condition that primarily affects the pilosebaceous units—structures comprising hair follicles and sebaceous (oil) glands. This condition is characterized by a variety of skin lesions, including non-inflammatory comedones and inflammatory papules, pustules, and, in more severe cases, nodules and cysts. Long-standing or untreated acne may result in permanent complications such as scarring and post-inflammatory hyperpigmentation.
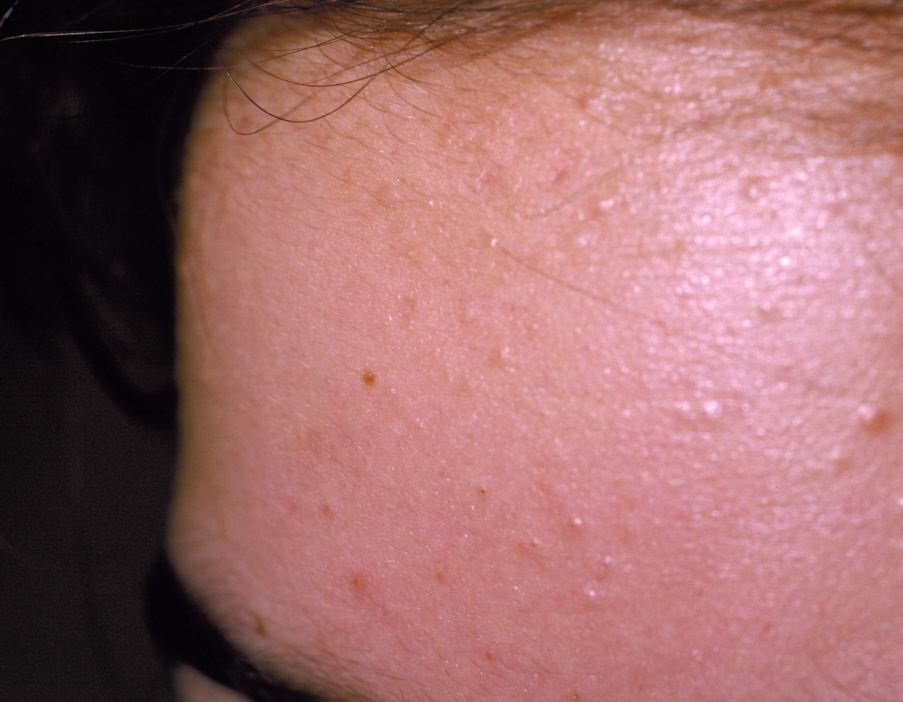
The typical areas affected by acne vulgaris are those rich in sebaceous glands: the face (especially the forehead, cheeks, and chin), the upper chest, the upper back, and the shoulders. These regions tend to produce more sebum, making them more susceptible to clogged pores and inflammation.
This form of acne is most commonly seen during adolescence, with symptoms beginning between ages 11 and 13. In boys, acne tends to appear slightly later—around 18–20 years old—and is generally more severe due to higher androgen levels. Girls typically experience earlier onset, though their cases tend to be milder in comparison. Acne vulgaris is not limited to teenagers, however; adult-onset acne is also common, particularly in women.
It is estimated that up to 80% of the global population experiences acne vulgaris at some point in life. Despite this high prevalence, many people still treat acne as a cosmetic issue rather than a medical one, often ignoring treatment until it becomes severe or leaves permanent marks on the skin.
The pathogenesis of acne vulgaris is multifactorial. It begins with the overproduction of sebum, followed by follicular hyperkeratinization, which leads to clogged pores. These blockages form comedones. If the blocked follicles become colonized by skin bacteria such as Cutibacterium acnes, the immune system responds, triggering inflammation and the progression to papules and pustules—hallmark features of inflammatory acne.
There is no single cause of acne vulgaris. Rather, it arises from a combination of internal and external factors. Understanding these triggers is key to tailoring effective treatment plans and preventing recurrences.
The diagnosis of acne vulgaris is clinical and typically straightforward. It is based on the visual assessment of lesions, their distribution, and the patient’s history. During a consultation, the dermatologist collects detailed information about the onset, evolution, severity, and any possible triggers or aggravating factors. This includes hormonal history, diet, stress levels, skincare habits, and use of medications.
On physical examination, the presence and dominance of specific lesion types—such as comedones, papules, pustules, or nodules—help define the form and severity of the acne. In ambiguous cases or in the presence of atypical or isolated lesions, dermatoscopy may be employed to rule out other dermatoses.
A thorough diagnosis not only allows for proper classification (mild, moderate, or severe acne) but also facilitates the identification of underlying contributing factors, enabling a more targeted and personalized treatment plan.
Acne vulgaris typically presents with a combination of non-inflammatory and inflammatory lesions. The hallmark features include:
The most frequent locations for acne vulgaris include the forehead, cheeks, chin, upper back, chest, and shoulders. Acne in other areas is rare and may indicate another underlying condition.
To confirm the diagnosis of acne vulgaris, dermatologists may need to differentiate it from other skin conditions with similar features. These include:
Although acne vulgaris is not a dangerous disease, it reflects underlying biological and environmental processes. These may include hormonal changes, immune dysregulation, or metabolic shifts. Ignoring these signals can delay the diagnosis of more significant health issues.
Acne also has serious psychosocial implications. Many patients—especially adolescents and young adults—experience reduced self-confidence, social isolation, anxiety, and even depression. The formation of scars and pigmentation changes can lead to long-lasting aesthetic concerns that affect quality of life.
Furthermore, untreated or poorly managed acne can lead to secondary bacterial infections, painful cysts, or abscess formation. Picking or squeezing lesions increases the risk of trauma, infection, and post-acne scarring.
Early and consistent dermatological care is essential to avoid complications. Patients should consult a dermatologist if:
Dermatologists can provide a structured treatment approach tailored to the patient’s skin type, acne severity, and lifestyle. Preventive consultations are especially important before major life changes (e.g., starting hormonal treatments, changing diets or cosmetics, or moving to different climates).
The treatment of acne vulgaris should be individualized and include a combination of therapeutic strategies. The most effective plans often combine both topical and systemic treatments along with supportive skincare routines. Key modalities include:
Patients must commit to treatment regimens for several months before significant improvement is seen. Skipping doses, using inappropriate products, or prematurely ending therapy can undermine progress and lead to recurrence.
While acne vulgaris cannot always be prevented, the following practices can reduce the frequency and severity of breakouts:
With professional guidance and disciplined self-care, acne vulgaris can be effectively managed, and long-term skin damage can be avoided—helping individuals maintain not only healthy skin, but also emotional well-being and confidence.