Acral Nevus (also known as benign nevus of the palms and soles, pigmented nevus of the palms and soles) is a benign skin growth that typically appears on the palms of the hands and soles of the feet. This type of nevus can be either acquired or congenital, but having multiple acral nevi on the same person is rare. Acral nevi make up about 5% of all pigmented nevi.
The exact cause of acral nevi is not fully understood, but there are factors that may contribute to their development or increase the risk of neoplasms:
The diagnosis of acral nevi is made through clinical examination, which includes a routine physical examination of the nevus and dermatoscopy. If malignancy is suspected, a biopsy may be performed.
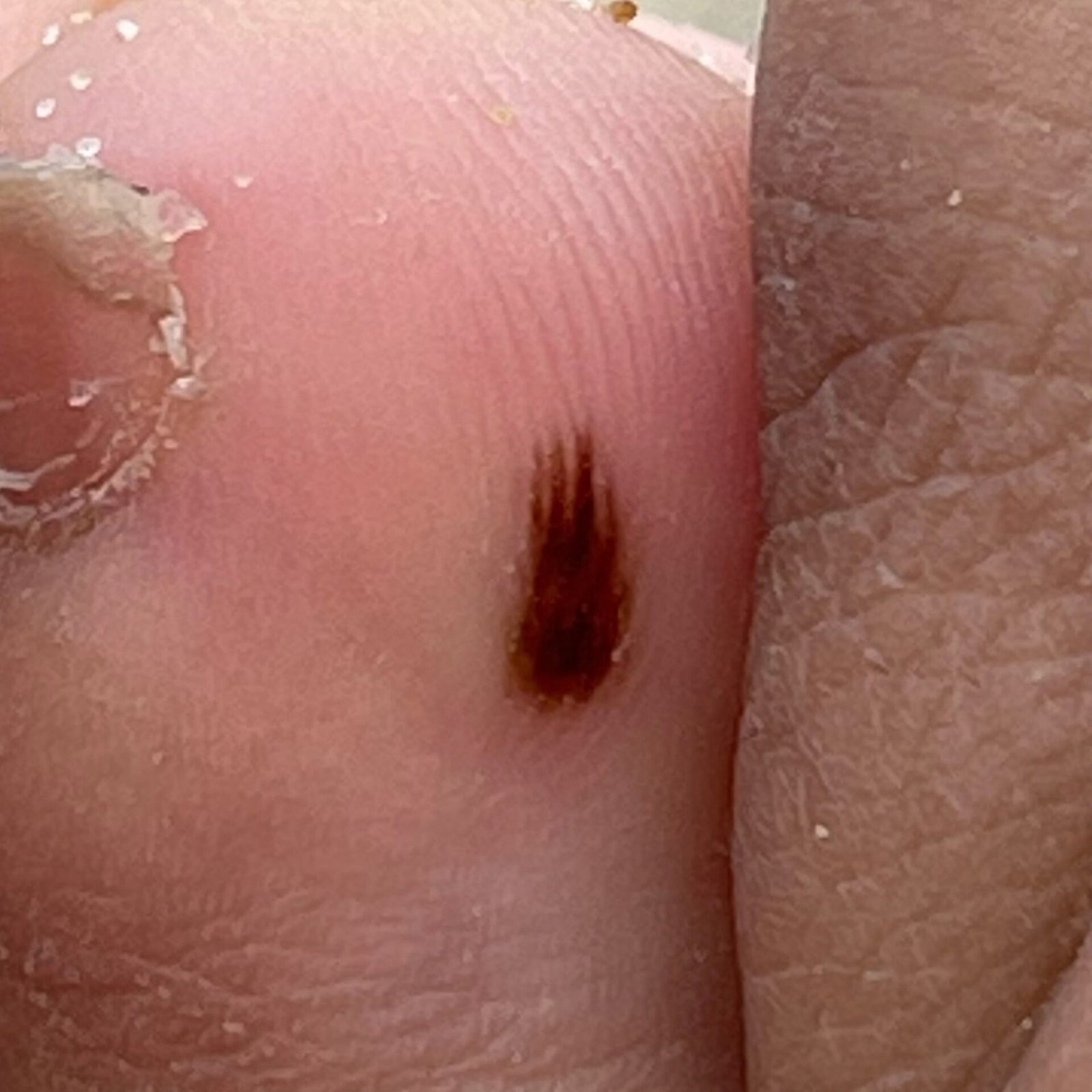
Acral nevi are found on the skin of the palms and soles. On visual examination, an acral nevus appears as a pigmented growth that is typically symmetrical (oval or round). The edges are usually irregular due to the natural skin pattern on the palms and soles. The texture of the nevus is either the same as the surrounding skin or slightly rough.
The color of acral nevi ranges from yellow-brown to dark brown (almost black), with the pigment evenly distributed throughout. Sometimes, the color intensity gradually decreases from the center to the outer edges.
The size of acral nevi usually does not exceed 10 mm, most often ranging from 3 to 5 mm. Upon palpation, the consistency is similar to normal skin, and there are no subjective sensations.
On dermatoscopy, an acral nevus appears with the following features:
Acral nevi need to be differentiated from the following pigmented lesions:
Acral nevi are generally harmless and do not increase the risk of melanoma. In the absence of external factors such as trauma, ultraviolet light, or ionizing radiation, the risk of malignant transformation is low and similar to that of unchanged skin. However, changes in appearance or the development of discomfort can indicate the possibility of malignancy.
Although acral nevi are typically safe, their appearance (irregular pigmentation, uneven edges, and linked structures) can sometimes resemble that of melanoma, particularly acral lentiginous melanoma. Therefore, newly detected acral nevi should be closely monitored to avoid missing an early melanoma form.
If there are no external factors impacting the acral nevus, and there are no changes in its appearance or subjective sensations, periodic self-monitoring (or monitoring by others for hard-to-reach areas) is usually sufficient. This should be done at least once a year. However, if the nevus experiences trauma, excessive UV or ionizing radiation, or any changes in appearance or discomfort occurs, a visit to a dermatologist or oncologist is recommended.
The specialist will assess whether ongoing monitoring is needed, or if the nevus should be removed. Nevi that are constantly irritated by clothing, jewelry, or occupation may also need to be removed.
Photographic documentation of the nevus can be very helpful for future comparisons, allowing even minor changes to be detected. Additionally, creating a map of skin neoplasms can simplify ongoing monitoring and identification of new or altered growths.
The treatment of acral pigmented nevi is purely surgical, using methods like classic excision, electrosurgery, or radiosurgery, followed by histological examination.
Destructive methods, such as laser removal or cryosurgery, are not recommended for treating acral nevi.
The prevention of nevi formation and their malignant transformation involves gentle care of the skin:
Regular checks of acral nevi, timely consultation with a specialist when changes occur, and removal of potentially dangerous nevi are essential for maintaining skin health.