Actinic Keratosis (also known as solar keratosis) is a benign skin tumor that appears as a rough, hyperemic spot with keratinization. This condition is most commonly observed in individuals over the age of 40, particularly in areas of the skin frequently exposed to solar ultraviolet (UV) radiation. Actinic keratosis is considered a precancerous condition, as it carries a significant risk of transforming into squamous cell carcinoma of the skin. The incidence of actinic keratosis increases with age, and it is characterized by its multiplicity, with new lesions appearing over time. Both men and women are equally affected by this condition.
Although the exact cause of actinic keratosis is not fully understood, several factors are known to increase the risk of developing this condition. These factors primarily involve environmental and genetic influences that make the skin more susceptible to damage and subsequent lesion formation:
The diagnosis of actinic keratosis is based on a clinical examination, which includes a visual inspection of the lesions and dermatoscopic analysis to assess the characteristics of the skin lesions. If there is suspicion that the lesion may be malignant or atypical, a biopsy may be performed for further evaluation.
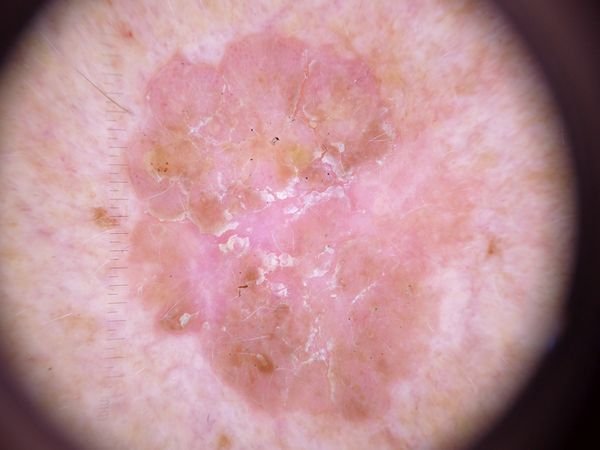
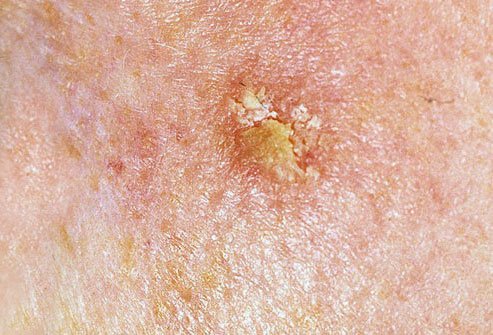
On visual examination, actinic keratosis presents as single or multiple flat or raised lesions with a rough, dry surface. These spots are typically covered with crusts and may show signs of erosion or bruising. The lesions often appear asymmetrical, with uneven, poorly defined borders. The color of the lesions varies, ranging from flesh-colored to gray, gray-brown, or pink. In some cases, the lesions may show redness surrounding the lesion, which is a common feature.
The size of actinic keratosis can vary from 5 mm to 20 mm, and grouped lesions may cover an area of 3-4 cm or more. The height of the lesions above the skin surface usually does not exceed 5-7 mm. These lesions typically do not affect hair growth, and in some cases, they can become itchy or uncomfortable, although subjective sensations are usually minimal.
Actinic keratosis most commonly affects sun-exposed areas of the skin, such as the face, ears, scalp, neck, upper limbs (particularly the shoulder girdle and wrists), and chest. The lesions are less commonly found on the palms and soles of the feet.
Dermatoscopy of actinic keratosis reveals several characteristic features that can help in the diagnosis:
Actinic keratosis must be differentiated from other skin lesions and conditions, including:
Actinic keratosis is considered a precancerous condition, with a significant risk of malignancy. The risk of transformation into squamous cell carcinoma (SCC) is estimated to be around 1-10%. In cases of malignancy, actinic keratosis can progress into squamous cell carcinoma, sometimes passing through an intermediate stage known as Bowen’s disease. Due to the cumulative effect of UV radiation, actinic keratosis lesions can increase in number and size over time, further raising the risk of malignant transformation.
Patients with severe actinic keratosis or large numbers of lesions may have an increased risk of developing other malignant tumors on unaffected skin areas, complicating the differential diagnosis and timely detection of skin cancer.
If there are no external factors causing changes in the appearance of the lesions or new symptoms such as pain or swelling, self-monitoring is typically sufficient. This should include regular checks, at least once a year, especially for lesions in hard-to-see areas. If the lesion experiences mechanical injury, is exposed to UV radiation, or if any changes are observed, a consultation with a dermatologist or oncologist is necessary.
A healthcare provider will determine whether further monitoring or removal of the lesions is necessary. Nevi that are subject to chronic trauma, such as from clothing, jewelry, or occupational activities, should be removed to prevent further irritation. It is also recommended to document any changes using photographs for dynamic observation.
Patients with multiple actinic keratoses should be evaluated by a dermatologist or oncologist in the spring and autumn (before and after periods of sun exposure). Creating a map of skin neoplasms can help with ongoing monitoring and identification of any new or altered lesions.
Treatment of actinic keratosis is necessary due to the risk of malignant transformation. If the underlying cause can be identified and treated, symptoms often resolve on their own. In idiopathic cases or when the cause remains unclear, symptomatic treatments may include:
Topical medications may also be used for treatment, including:
It is important that these treatments be administered under the supervision of a healthcare professional, as side effects and relapse are possible.
Prevention of actinic keratosis and its potential for malignancy involves careful management of sun exposure and skin health:
Regularly checking the skin for actinic keratosis, seeking timely consultation with a healthcare professional if changes occur, and removing potentially dangerous lesions are essential for maintaining skin health and preventing complications.