Basal Cell Carcinoma (BCC) is a malignant tumor of the skin that originates from the basal cells of the epidermis. It is characterized primarily by its locally invasive growth and its extremely low potential to metastasize to distant organs. Despite being malignant, BCC is considered the least aggressive form of skin cancer due to its rare association with systemic spread. However, if left untreated, the tumor can cause significant local tissue destruction, disfigurement, and functional impairment. The prognosis for BCC is generally favorable, particularly when diagnosed early and managed appropriately. BCC typically affects individuals over the age of 35–40 and occurs with roughly equal frequency in both men and women.
While there is no singular definitive cause for the development of basal cell carcinoma, several predisposing factors have been identified that significantly increase the likelihood of its occurrence. These risk factors often act cumulatively over time and are most relevant in individuals with prolonged environmental or occupational exposure:
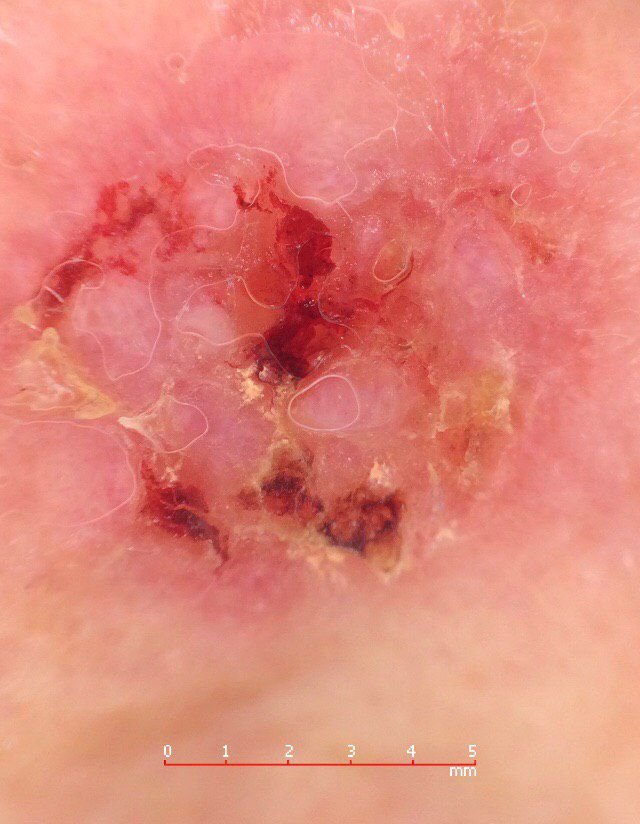
The diagnosis of basal cell carcinoma begins with a comprehensive clinical examination. The dermatologist evaluates the lesion’s morphology, surface characteristics, and behavior over time. Dermatoscopy is then used to enhance visualization of sub-surface features such as vascular patterns, pigmentation, and structural asymmetries. If clinical and dermatoscopic findings suggest malignancy, a skin biopsy is performed to confirm the diagnosis. This involves taking a sample of tissue from the lesion and examining it histologically for features specific to BCC, such as basaloid cell proliferation with peripheral palisading and stromal retraction.
Basal cell carcinoma typically presents as a slowly enlarging, raised lesion or plaque that may appear pink, flesh-colored, or red. Its surface may show signs of nodularity, wart-like growths, erosion, ulceration, or crusting. Bleeding can occur even with minor trauma or spontaneously due to the fragility of the neoplastic vasculature. The edges of the lesion are often poorly defined and infiltrative, reflecting its tendency to grow deep into the dermis and subcutaneous tissues.
In its classic form, BCC may resemble a small crater-like ulcer with rolled, pearly edges and a depressed central area. Alternatively, it may present as a protruding nodule fixed to the skin, sometimes on a broad base. The color can vary depending on the lesion’s stage: early forms are pink to red, while older or necrotic areas may appear white, yellowish, or gray. The lesion usually lacks hair growth due to follicular destruction.
The size of a basal cell carcinoma may range from 4 mm to over 40 mm. It grows slowly over months to years, but in the absence of treatment, it can expand significantly and infiltrate surrounding anatomical regions. The lesion is typically painless; however, if it invades deeper tissues such as nerves or muscle, pain or neurological symptoms may develop. The most common locations include sun-exposed areas such as the face (especially the nose, forehead, and cheeks), ears, scalp, neck, upper chest, shoulders, and forearms.
Dermatoscopy is a valuable tool in the assessment of basal cell carcinoma. Typical features visualized through dermatoscopy include:
The differential diagnosis for BCC includes a range of benign and malignant skin conditions that may mimic its clinical features. These include:
Although BCC is classified as a malignant tumor, its prognosis is generally favorable due to its extremely low rate of metastasis. The primary concern is local tissue destruction and recurrence after treatment. The risk of recurrence is influenced by the size, depth of invasion, and adequacy of initial treatment. Large tumors or those that were not fully excised have a higher chance of recurrence.
In addition to local recurrence, patients with BCC are at increased risk of developing subsequent skin cancers in other locations. Therefore, comprehensive skin surveillance is recommended. Clinical follow-up, photographic documentation, and total body skin mapping are essential for monitoring and early detection of new or changing lesions.
Recent studies have shown an increase in the incidence of BCC globally, with a roughly 10% rise over five years. This highlights the importance of awareness, early detection, and preventive strategies.
The mainstay of BCC treatment is complete surgical excision with clear margins, which ensures removal of the entire tumor and reduces the risk of recurrence. This is considered the gold standard for most types of BCC.
Other treatment options include:
Destructive procedures such as cryotherapy or laser removal are generally discouraged for BCC due to the lack of histological confirmation and higher risk of incomplete removal.
Preventive strategies focus on minimizing UV-induced skin damage and identifying early signs of skin cancer. Effective prevention includes:
Timely consultation with a dermatologist or oncologist in the presence of suspicious skin changes is critical to prevent complications and ensure effective treatment.