Bowen’s Disease, also known as squamous cell carcinoma in situ (SCC in situ), is an early form of skin cancer. It presents as a persistent red or pink patch or plaque with a rough, scaly surface. Unlike invasive squamous cell carcinoma, Bowen’s disease is confined to the epidermis and has not yet penetrated the basement membrane. This non-invasive nature gives Bowen’s disease a favorable prognosis when detected and treated promptly. The condition is typically observed in individuals over the age of 35–40 and occurs slightly more frequently in women.
While the exact cause of Bowen’s disease remains uncertain, several factors have been identified that increase susceptibility. These include environmental exposures, chronic skin damage, and underlying dermatological conditions:
Diagnosis begins with a clinical examination of the lesion. The physician evaluates the morphology, surface characteristics, and behavior over time. Dermatoscopy is used to enhance visualization of vascular structures and surface texture. If malignancy is suspected, a skin biopsy is performed to confirm the diagnosis and assess the depth of cellular involvement.
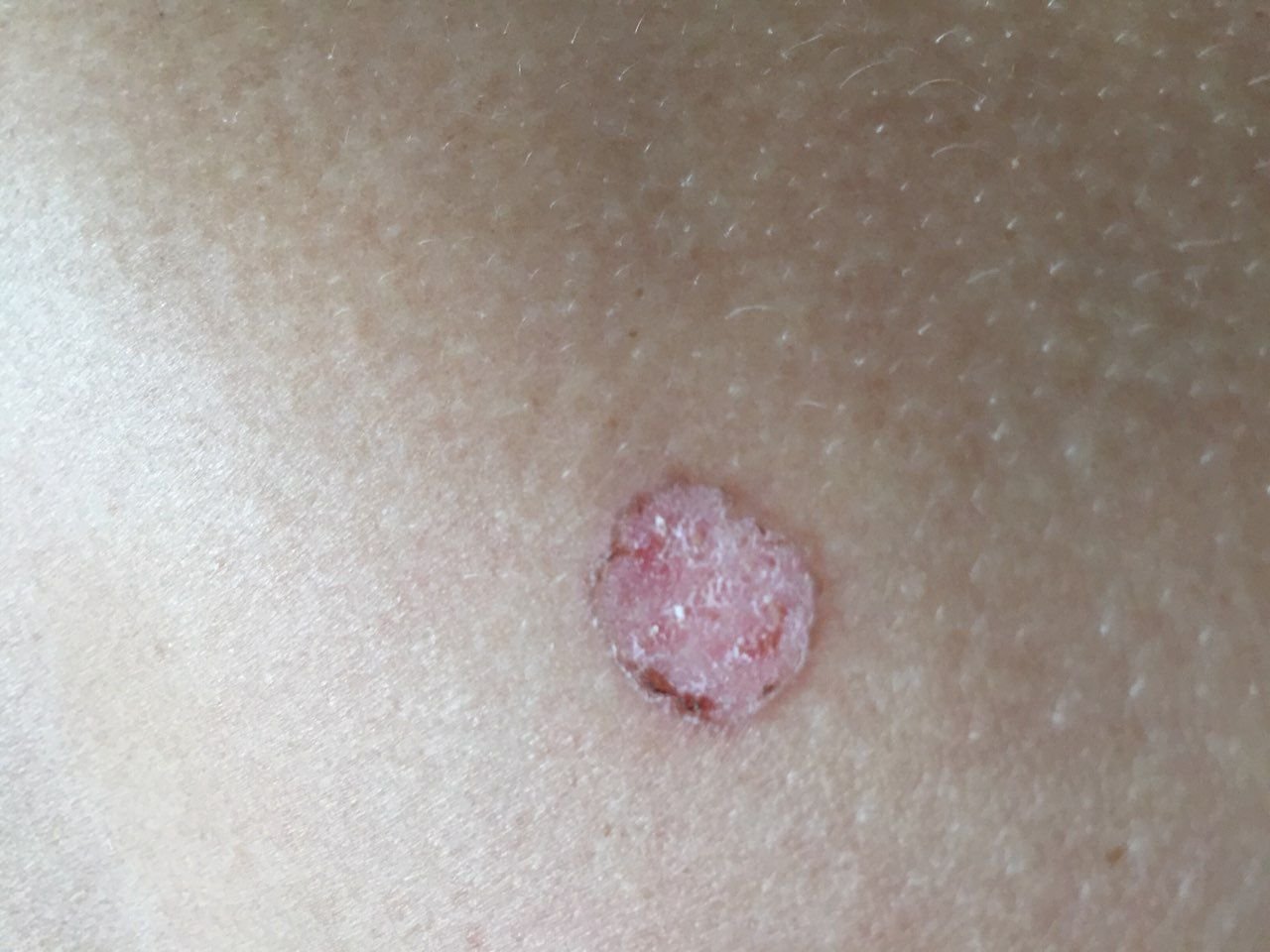
Bowen’s disease typically presents as a solitary, persistent, well-demarcated erythematous patch or plaque. In rare cases, multiple or grouped lesions may be observed. The surface may be rough, scaly, crusted, or exhibit wart-like growth. Signs of erosion or ulceration may also be present. The lesion usually remains flat or slightly elevated (≤1 mm), with edges that may be more prominent.
The shape of the lesion is often irregular and asymmetric. The coloration ranges from pink to reddish, and with the presence of keratinization, shades of gray may appear. Hair is absent in the lesion area. Sizes vary from 4 mm to 40 mm or more in grouped lesions. Growth is slow and steady, with no spontaneous regression. On palpation, the lesion feels firmer than surrounding skin and may peel easily. Removal of crusts reveals an eroded, reddened surface. Patients may report mild itching or burning, though many are asymptomatic.
Common sites include sun-exposed areas such as the face, scalp, neck, shoulders, arms, and torso.
Under dermatoscopic examination, Bowen’s disease reveals several distinctive features:
Bowen’s disease must be differentiated from a variety of benign and malignant skin conditions, including:
Bowen’s disease is a form of non-invasive squamous cell carcinoma (carcinoma in situ), which means that malignant cells are confined to the epidermis and have not invaded deeper layers of the skin. The absence of basement membrane penetration makes the prognosis excellent if treated in time. However, if left untreated, Bowen’s disease has the potential to evolve into invasive squamous cell carcinoma, which may then metastasize and become life-threatening.
Because of this risk, some oncological classifications treat Bowen’s disease as an obligate precancerous condition — a state that, without intervention, will eventually progress to invasive cancer. This highlights the importance of early diagnosis and appropriate treatment.
When Bowen’s disease is suspected, patients should be promptly referred to an oncologist or dermatologist for further evaluation. If the lesion cannot be diagnosed definitively by visual or dermatoscopic means, a biopsy or complete excision is performed for histological confirmation. Once confirmed, a tailored treatment plan is developed based on lesion size, location, and patient factors.
Since patients with Bowen’s disease have a higher risk of developing other cutaneous malignancies, regular full-body skin checks are essential. Suspicious lesions should be photo-documented to aid in future comparisons. Skin mapping (total body photography) is often recommended for individuals with multiple lesions or extensive sun damage. Routine dermatological evaluations are typically advised in spring and autumn, particularly surrounding periods of increased UV exposure.
The mainstay of treatment is surgical excision with clear margins. This method is preferred due to its high efficacy and low recurrence rates. It also allows for histopathological confirmation of complete lesion removal.
Other treatment options include:
Preventing Bowen’s disease and its progression to invasive carcinoma involves minimizing exposure to harmful environmental factors and monitoring the skin regularly. Key preventive strategies include: