Eczema: Chronic Inflammatory Skin Disorder with Diverse Clinical Forms
Overview
Eczema is a non-infectious, inflammatory skin condition characterized by intense itching, redness, peeling, and polymorphic rashes, which can appear in the form of vesicles, crusts, or lichenified plaques. Eczema can present in acute or chronic forms and often follows a cyclical course with seasonal exacerbations—worsening in cold months and improving in warm seasons.
This condition affects people of all ages and is not transmitted through contact. It may develop due to a combination of genetic, immune, environmental, and lifestyle-related factors. Eczema is one of the most common reasons for dermatological consultations worldwide.
Etiology and Risk Factors
The development of eczema is multifactorial. It is often associated with an inherited tendency to develop hypersensitivity reactions (atopy), but can also be triggered by external irritants, internal diseases, or immune dysregulation.
Primary causes:
- Genetic predisposition (e.g., family history of eczema, asthma, or allergies);
- Compromised skin barrier function;
- Dysfunction of immune response and overactive inflammation pathways.
Secondary/external contributing factors:
- Chronic stress and emotional overload;
- Endocrine or gastrointestinal disorders;
- Decreased immunity;
- Hyperhidrosis (excessive sweating);
- Varicose veins and circulatory disorders;
- Chronic infections or microbial imbalances;
- Exposure to household chemicals, perfumes, cosmetics, or unsuitable topical agents.
Clinical Classification of Eczema
Eczema is classified into several types based on etiology, clinical features, and location. Each form has its own triggers and progression pattern. Common clinical types include:
- True (idiopathic) eczema
- Seborrheic eczema
- Dyshidrotic eczema
- Microbial eczema
- Hypostatic (varicose) eczema
- Occupational eczema
- Children’s (infantile) eczema
True (Idiopathic) Eczema
- Characterized by symmetrical inflammatory lesions with indistinct borders;
- Manifested by vesicles, serous exudation, erosions, crusts, and scaling;
- Intense itching and burning are typical;
- Often starts on the face and hands, spreading to other body areas over time;
- In chronic forms, the skin becomes thickened, lichenified, and cracked.
Seborrheic Eczema
- Occurs in individuals with oily skin and overactive sebaceous glands;
- Primarily affects the scalp, behind the ears, face (nasolabial folds), neck, and upper chest;
- Lesions present as yellowish-pink nodules, crusts, and oily scaling on erythematous skin;
- Scalp may show sticky hair with exudate and greasy crusts;
- Itching is often present, especially in body folds.
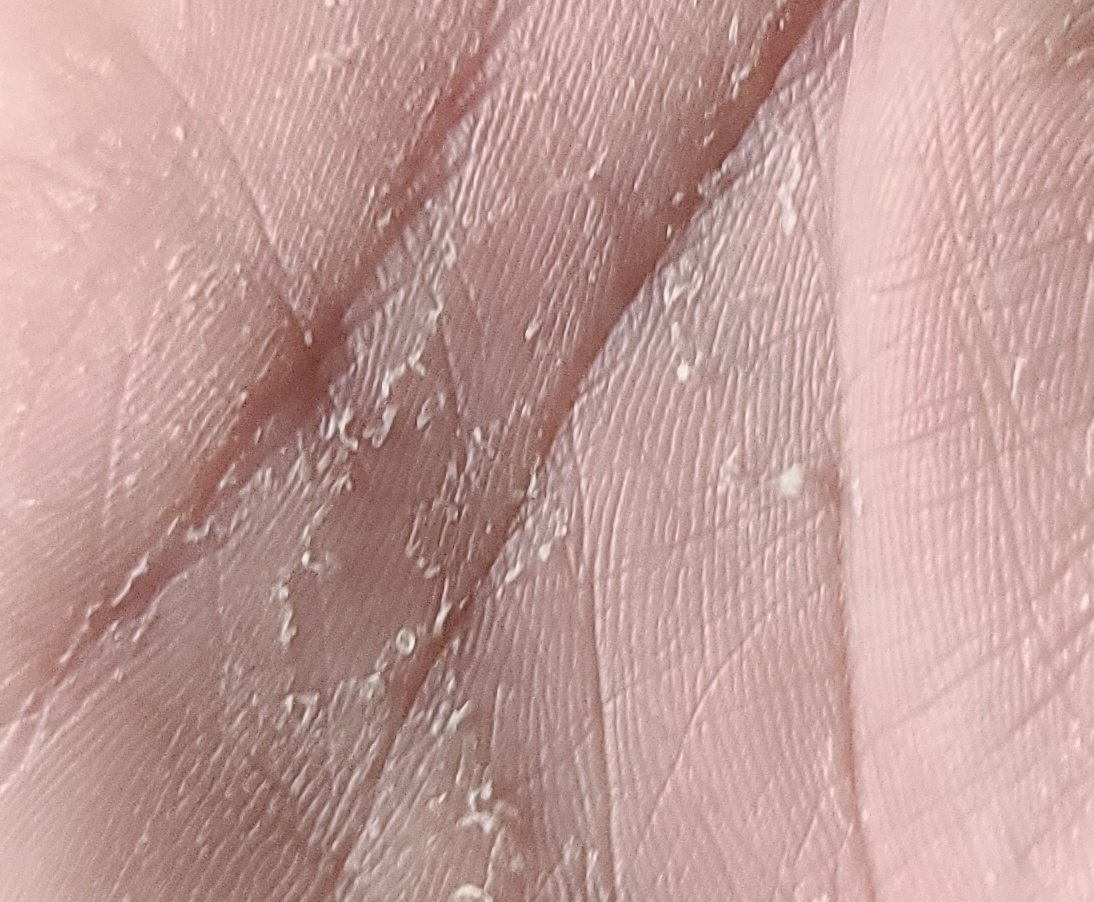
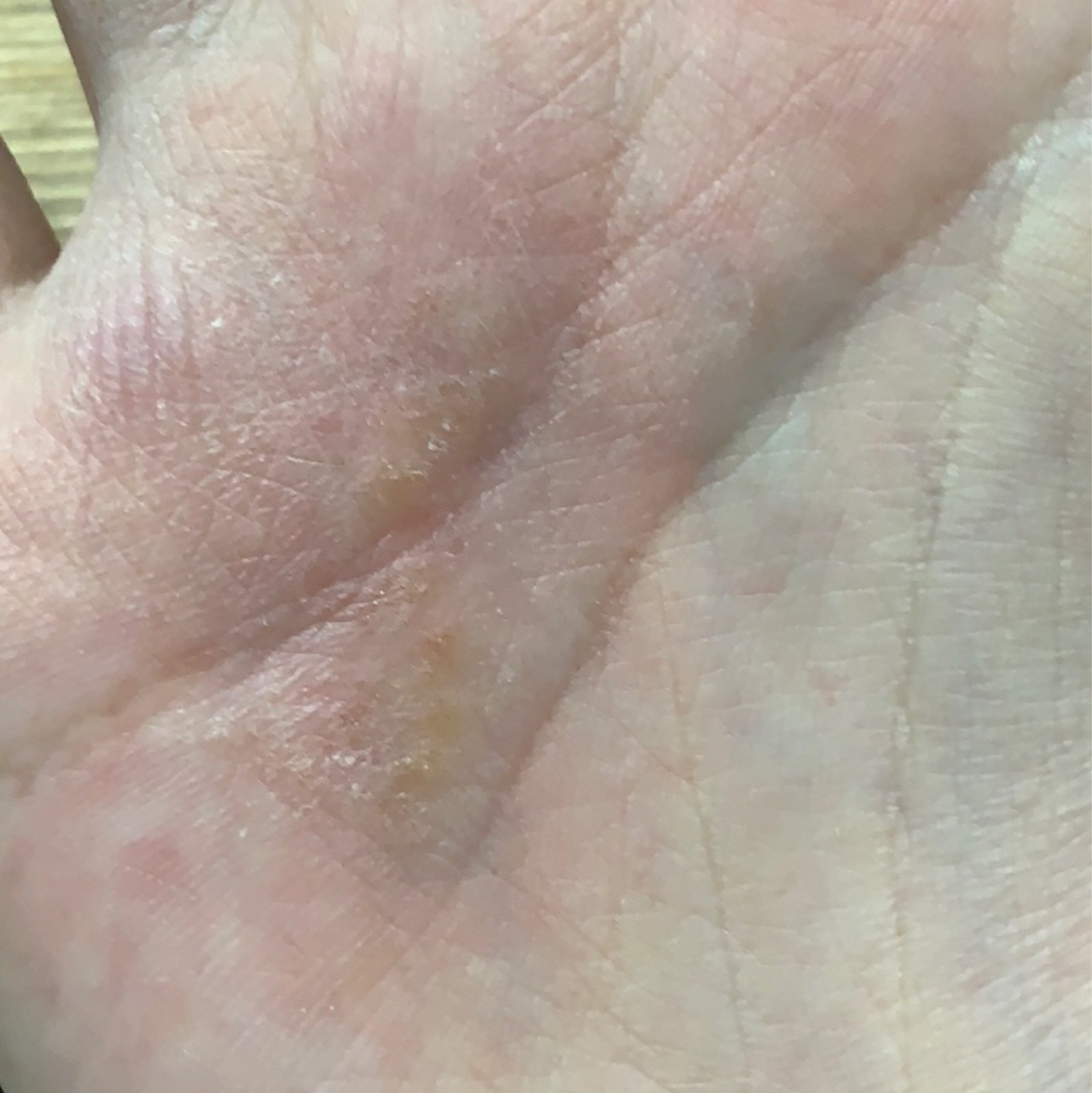
Dyshidrotic Eczema
- Primarily affects palms, soles, and lateral aspects of fingers;
- Triggered by allergic responses, emotional stress, or seasonal factors (spring/summer);
- Small, deep-seated clear vesicles evolve into erosions with peeling and discomfort;
- Burning and soreness may accompany flare-ups;
- Adults under 40 are most affected, though rare in children.
Nummular (Discoid) Eczema
- Characterized by round or oval plaques resembling coins (hence the term “nummular”);
- Lesions may be exudative or dry, and are often intensely itchy;
- Commonly affects shins, forearms, and back of hands;
- Often provoked by dry skin, insect bites, nickel allergy, poor circulation;
- Seen more frequently in men, particularly middle-aged and elderly individuals.
Microbial Eczema
- Occurs when the skin becomes hypersensitive to microbial antigens (e.g., staphylococcus, streptococcus);
- Often arises around chronic wounds, ulcers, or varicose veins;
- Lesions have clear borders, purulent crusts, and underlying moist areas;
- Itching is prominent, and lesions may spread if untreated;
- Can accompany systemic conditions such as immune or endocrine dysfunction.
Hypostatic (Varicose) Eczema
- Associated with venous insufficiency, varicose veins, heart or kidney failure, obesity, or diabetes;
- Primarily affects lower legs and ankles;
- Patients experience heaviness, pain, swelling, and redness;
- Serous-purulent crusts form over inflamed, edematous skin;
- Often complicated by secondary infection or ulceration.
Diagnostics
Eczema is usually diagnosed clinically by a dermatologist. In complex cases or chronic forms, additional tests help to identify triggers and exclude other skin conditions.
Diagnostic methods include:
- Clinical examination: Pattern, distribution, and history of symptoms;
- Allergy testing: Patch or skin prick tests to detect contact allergens or atopic triggers;
- Blood tests: Total and specific IgE, eosinophil count, inflammatory markers;
- Microscopic analysis: KOH test to rule out fungal infection;
- Skin scrapings and cultures: In suspected microbial eczema;
- Biopsy: In uncertain cases to distinguish from psoriasis, cutaneous lymphoma, or dermatitis herpetiformis.
Differential Diagnosis
Conditions that may resemble eczema include:
- Allergic contact dermatitis;
- Atopic dermatitis;
- Psoriasis (especially inverse or guttate forms);
- Seborrheic dermatitis;
- Scabies or fungal infections (tinea);
- Drug reactions (toxicoderma);
- Pyoderma and impetigo (especially in microbial eczema).
Treatment
Management of eczema involves a comprehensive approach focused on inflammation control, itch relief, skin barrier restoration, and avoidance of triggers. A dermatologist provides a tailored treatment plan based on type and severity.
Core treatment principles:
- Topical therapy: Corticosteroids, calcineurin inhibitors, antiseptic solutions, moisturizers;
- Systemic therapy (if indicated): Antihistamines, antibiotics (for secondary infections), corticosteroids, immunosuppressants (in chronic severe eczema);
- Physical therapy: UV therapy, baths with antiseptics, ozone therapy in selected cases;
- Identification and elimination of triggers: Allergen avoidance, psychological support, treating underlying diseases (e.g., varicosities, digestive disorders);
- Diet and lifestyle: Hypoallergenic diet, skin-friendly clothing, proper hydration, regular moisturizing;
- Rational use of medical cosmetics: pH-balanced cleansers, fragrance-free emollients, barrier repair creams.
Prevention
While eczema cannot always be prevented, recurrence and exacerbation can be minimized by:
- Maintaining a regular skincare routine and moisturizing daily;
- Using non-irritating, hypoallergenic personal care products;
- Protecting skin from trauma, excessive washing, and environmental extremes;
- Avoiding known allergens and triggers identified through diagnostic tests;
- Managing comorbidities such as stress, GI disorders, hormonal imbalance, and chronic infection;
- Wearing cotton clothing and avoiding synthetic or wool materials directly on the skin;
- Limiting hot showers and using gentle cleansers;
- Seeking timely dermatological advice if new or worsening symptoms occur.
Conclusion
Eczema is a heterogeneous group of inflammatory skin diseases with variable etiology and manifestations. Though often chronic and prone to relapse, most forms are manageable with individualized care, early intervention, and ongoing skin maintenance. With patient education, trigger avoidance, and proper dermatological support, individuals with eczema can achieve long-term control and improved quality of life.