Halo Nevus (also known as Sutton’s Nevus) is a benign skin neoplasm that typically appears as a raised spot surrounded by a rim of hypopigmented skin, creating a characteristic “halo” effect. Most commonly, halo nevi are first observed in individuals between the ages of 15 and 25, starting as a pigmented central area with a gradually expanding colorless ring around it. Over time, the central pigmented part of the nevus may undergo involution, either fading into hypopigmentation or completely disappearing after a period of 3 to 4 years, leaving only the surrounding hypopigmented ring.
Although the exact cause of halo nevus remains unclear, several predisposing factors are believed to influence the likelihood of its appearance. These factors may contribute to an increased risk of the development of halo nevi:
The diagnosis of halo nevus is primarily based on a thorough clinical examination. This includes a visual assessment of the lesion and dermatoscopic evaluation to closely inspect its structure and characteristics. If there are concerns about the possibility of malignant transformation, a biopsy may be necessary to confirm the benign nature of the lesion and exclude other conditions.
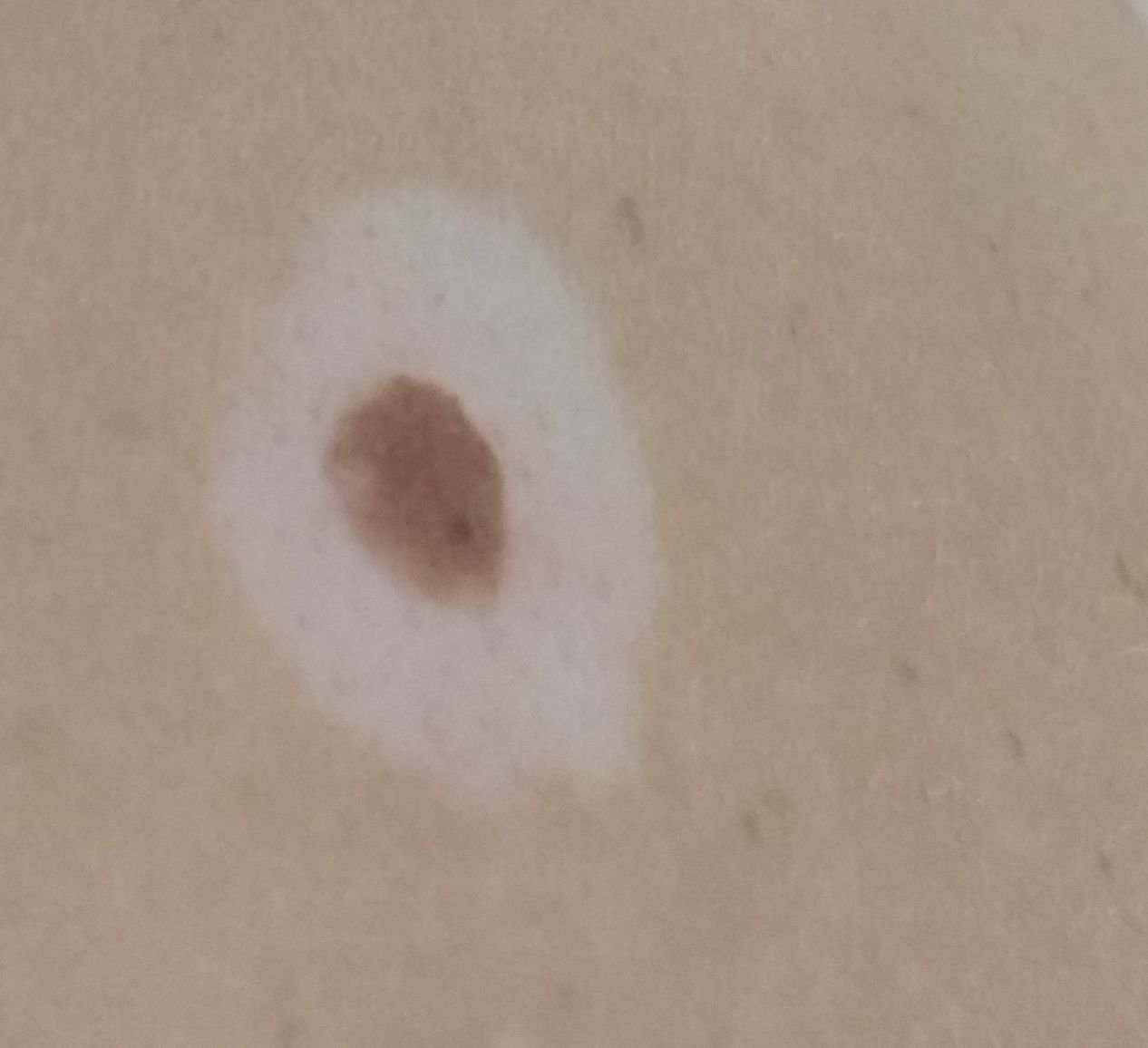
When visually examined, a halo nevus presents as a hemispherical or slightly raised formation, often symmetrical in shape (commonly oval or round). Surrounding the central pigmented area, there is a noticeable ring of hypopigmented skin. This colorless ring typically has a regular oval or round shape and is symmetrical in appearance.
The surface of the central pigmented area of the nevus may appear slightly different from that of the surrounding skin, with a smoother texture or a finely tuberous surface. The skin pattern of the depigmented ring remains unchanged and follows the natural texture of the skin.
The edges of the halo nevus are generally clear and well-defined. The central pigmented area may range in color from flesh-colored or tan to dark brown, with pigment uniformly distributed across the lesion. Sometimes, the intensity of the color gradually decreases from the center towards the periphery, or various shades of the same color may be present within the central area. The surrounding rim is typically colorless, although it can occasionally be light brown or pale pink, sometimes with slight hyperemia. The color of the hypopigmented ring becomes more noticeable and contrasting, especially after tanning.
The presence of a halo nevus does not generally affect hair growth. However, in some cases, the central part of the nevus may have a small amount of coarse bristly or fluffy hair.
The diameter of the central pigmented part of the halo nevus is usually small, not exceeding 10 mm. The total diameter, including the surrounding depigmented ring, can reach 3-4 cm. Over time, the size of the depigmented area may change, either increasing or decreasing. The height of the raised part of the nevus above the skin’s surface typically does not exceed 3-4 mm.
Upon palpation, the halo nevus feels like normal skin or may be slightly softer, particularly in the central pigmented area. There are no subjective sensations associated with the lesion, although mild itching may occasionally occur in rare instances.
Halo nevi are most commonly located on the body, particularly the trunk, but they can occasionally be found on other parts of the body as well.
During dermatoscopy of the central pigmented area of the halo nevus, the following features can typically be observed:
When dermatoscopically examining the depigmented area, it typically appears as normal skin with little to no pigment structures, though a subtle vascular network may be visible.
Halo nevus should be differentiated from other skin lesions and conditions, including:
Halo nevi are generally safe and do not pose a significant risk of developing into melanoma. In the absence of external factors such as trauma, UV radiation, or ionizing radiation, the risk of malignancy is comparable to the risk of skin cancer in unchanged skin. However, signs of potential malignancy include changes in the appearance of the nevus, as well as the appearance of new sensations such as itching, pain, or tenderness.
While the risk of melanoma in halo nevi is low, it can be slightly higher compared to other types of benign nevi. Changes in the appearance or behavior of the nevus should be carefully monitored, particularly in individuals with multiple moles.
For halo nevi that do not show signs of damage or significant changes in appearance, self-monitoring is generally sufficient. This includes regular checks, with assistance from others to examine hard-to-reach areas, at least once a year. If the nevus experiences mechanical damage, changes in its appearance occur, or new sensations such as pain or itching develop, a dermatologist or oncologist should be consulted immediately.
The healthcare provider will assess whether further dynamic monitoring is needed or if the nevus should be removed. Nevi that are subject to chronic trauma from clothing, jewelry, or occupation should be removed to prevent further irritation or potential complications.
For those undergoing dynamic observation, photographing the nevus is highly recommended, as it will help detect even minor changes in its appearance over time. Patients with multiple nevi should be evaluated by a dermatologist or oncologist in the spring and autumn (before and after sun exposure) to assess any changes. Maintaining a map of skin neoplasms can be a valuable tool for monitoring and identifying new or altered lesions.
The only recommended treatment for halo nevus is surgical excision, performed with either a classic scalpel or a radiofrequency scalpel. A histological examination of the excised tissue is necessary to ensure the lesion is benign.
Destructive methods such as laser removal or cryodestruction are not recommended for halo nevi due to the risk of relapse and incomplete removal.
Preventing the appearance of halo nevi and minimizing their risk of malignancy requires careful skin care:
It is essential to regularly inspect halo nevi, seek prompt consultation with a healthcare professional if any changes are noticed, and remove potentially dangerous lesions when needed.