Lentigo melanoma is a distinct form of malignant melanoma that originates from melanocytes — the pigment-producing cells responsible for melanin synthesis in the skin. This tumor most often arises in individuals over the age of 50 and typically affects areas chronically exposed to ultraviolet radiation, such as the face, neck, ears, and scalp. Lentigo melanoma commonly evolves from a long-standing pigmented lesion known as lentigo maligna (also referred to as Dubreuilh’s melanosis), which is considered a precancerous condition. Although it represents a relatively small percentage of all melanoma cases — about 5% — this subtype is considered clinically significant due to its potential for local invasion, recurrence, and eventual metastasis.
Unlike nodular melanoma, which is known for rapid vertical growth, lentigo melanoma initially expands slowly in a radial pattern along the skin’s surface. However, despite its indolent onset, it is regarded as aggressive due to its high recurrence rate and potential to spread via both lymphatic and hematogenous routes. Over time, the tumor may invade deeper skin layers and reach nearby lymph nodes or distant organs such as the lungs, liver, bones, or brain. The overall progression of the disease is strongly influenced by the patient’s immune response, emphasizing the need for early diagnosis and appropriate treatment.
Lentigo melanoma is rarely diagnosed in younger individuals and is closely associated with chronic UV damage. Risk factors that contribute to its development include:
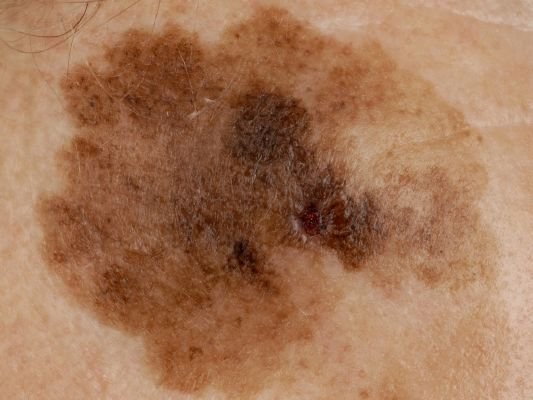
The diagnostic process begins with a detailed skin examination by a dermatologist, including dermatoscopic analysis. Lesions suspected of being lentigo melanoma are assessed using the ABCDE rule, which helps identify signs of malignancy:
Confirmation of the diagnosis is only possible through histopathological evaluation of a biopsy sample. Advanced imaging (e.g., ultrasound, CT, MRI, or PET) may be required to assess for metastasis.
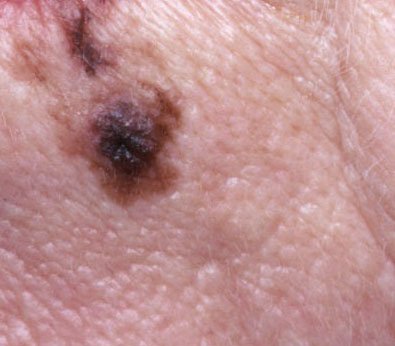
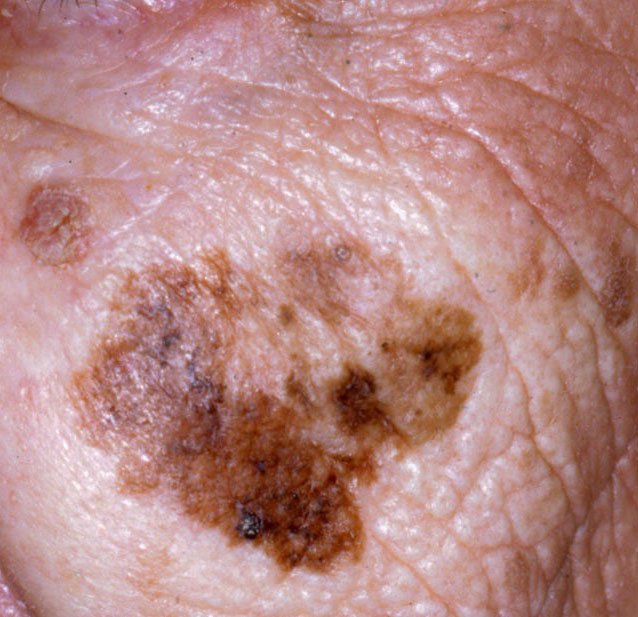
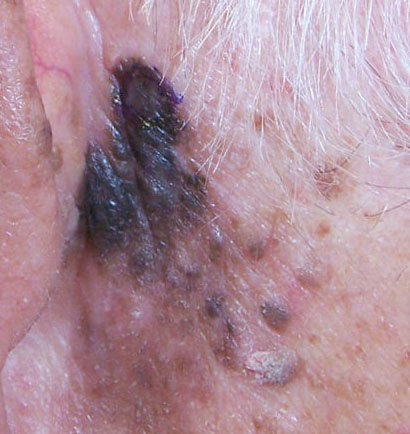
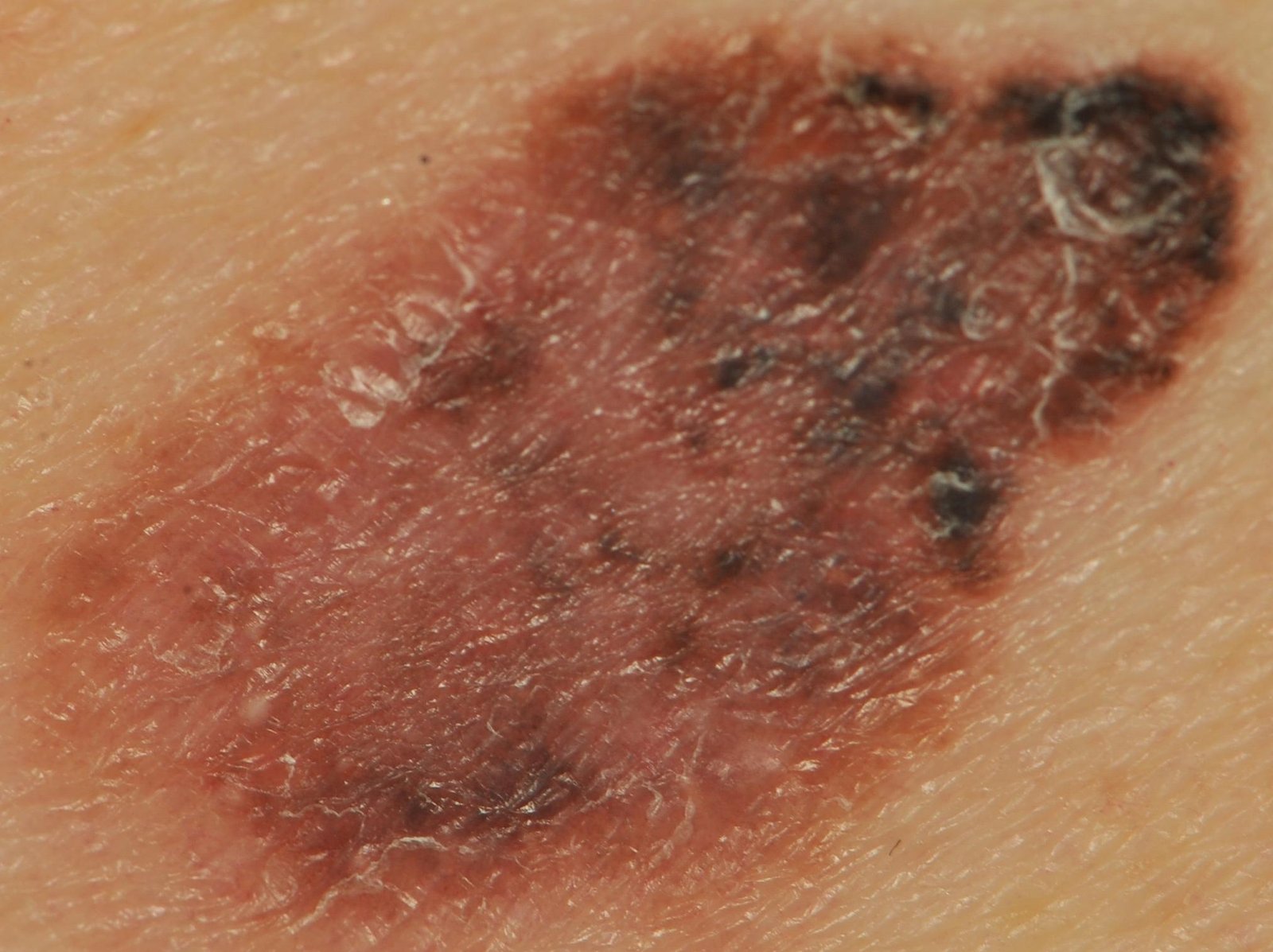
In the early stages, lentigo melanoma may appear as a slowly expanding, irregularly pigmented macule. Initially asymptomatic, it may go unnoticed for years. Over time, however, the lesion can darken, develop uneven borders, and change in texture. Symptoms and visible changes that often prompt medical attention include:
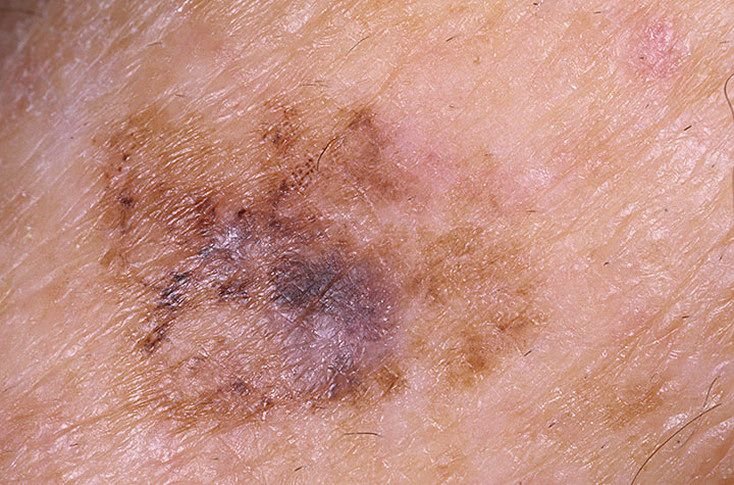
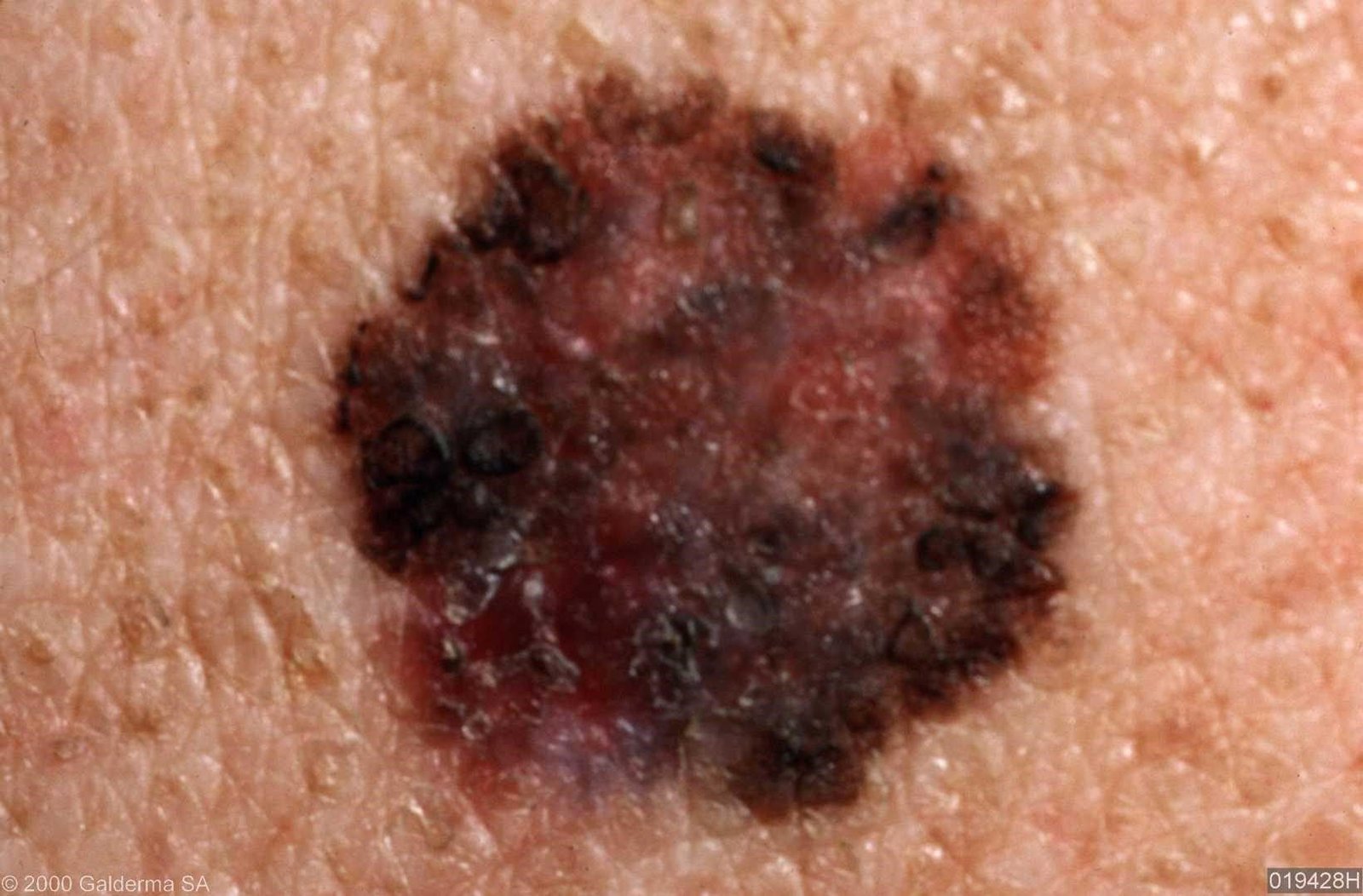
Dermatoscopy significantly enhances diagnostic accuracy by revealing characteristic subsurface features of lentigo melanoma. Common findings include:
Several skin lesions can mimic lentigo melanoma, making differential diagnosis critical. Conditions to consider include:
Although melanoma comprises a smaller fraction of skin cancer cases overall, it is responsible for a disproportionately high number of skin cancer-related deaths. Lentigo melanoma, in particular, may go undetected for years due to its slow onset and resemblance to benign pigmented lesions. The longer the diagnosis is delayed, the greater the risk of dermal invasion and metastatic spread.
When detected and treated early — before the vertical growth phase — lentigo melanoma has a comparatively favorable outcome. However, once metastasis occurs, the prognosis becomes significantly poorer. Regular monitoring and early intervention are essential to reduce mortality.
Suspected lentigo melanoma should be urgently referred for specialist evaluation. Excisional biopsy is preferred to obtain a complete tissue sample for histopathological review. Once confirmed, staging investigations are performed to assess lymph node involvement and identify possible distant metastases. These include clinical palpation, ultrasound, and cross-sectional imaging (e.g., CT, MRI, PET).
Ongoing surveillance with digital dermatoscopy and periodic full-body skin exams is strongly recommended for patients with high-risk lesions or a history of melanoma.
The cornerstone of treatment is wide surgical excision with histologically confirmed clear margins. In cases where regional lymph nodes are involved, a lymphadenectomy may be performed. For metastatic disease, treatment options are tailored to the individual and may include:
Important: Superficial removal methods, including cryotherapy, laser therapy, or shave excision, are contraindicated as they do not guarantee complete tumor clearance and prevent proper histological assessment.
Preventing lentigo melanoma involves long-term vigilance and minimizing UV damage. Recommended strategies include:
Early recognition and prompt removal of suspicious lesions are crucial steps in preventing disease progression and improving long-term outcomes.