Linear lichen, also known as acquired linear lichenoid dermatosis, Blaschko’s lichen, or Blaschkoid inflammatory rash, is a rare, benign inflammatory skin disorder characterized by the appearance of small, flat-topped papules that follow the embryonic lines of Blaschko. This condition is typically self-limiting and often requires no specific treatment.
Linear lichen most frequently develops in children aged 5 to 15 years, though it may occur at any age. In early childhood (under 3 years), the disease tends to affect boys slightly more often, although this gender predominance is not consistent in older children and adults.
The exact cause of linear lichen remains unclear. It is generally classified as an idiopathic dermatosis, though several internal and environmental factors are considered possible triggers. Its distribution pattern along Blaschko’s lines suggests an embryologic origin and possible involvement of cutaneous mosaicism or autoimmune phenomena.
The immune hypothesis suggests a localized autoimmune reaction in genetically predisposed individuals, potentially initiated during embryonic development.
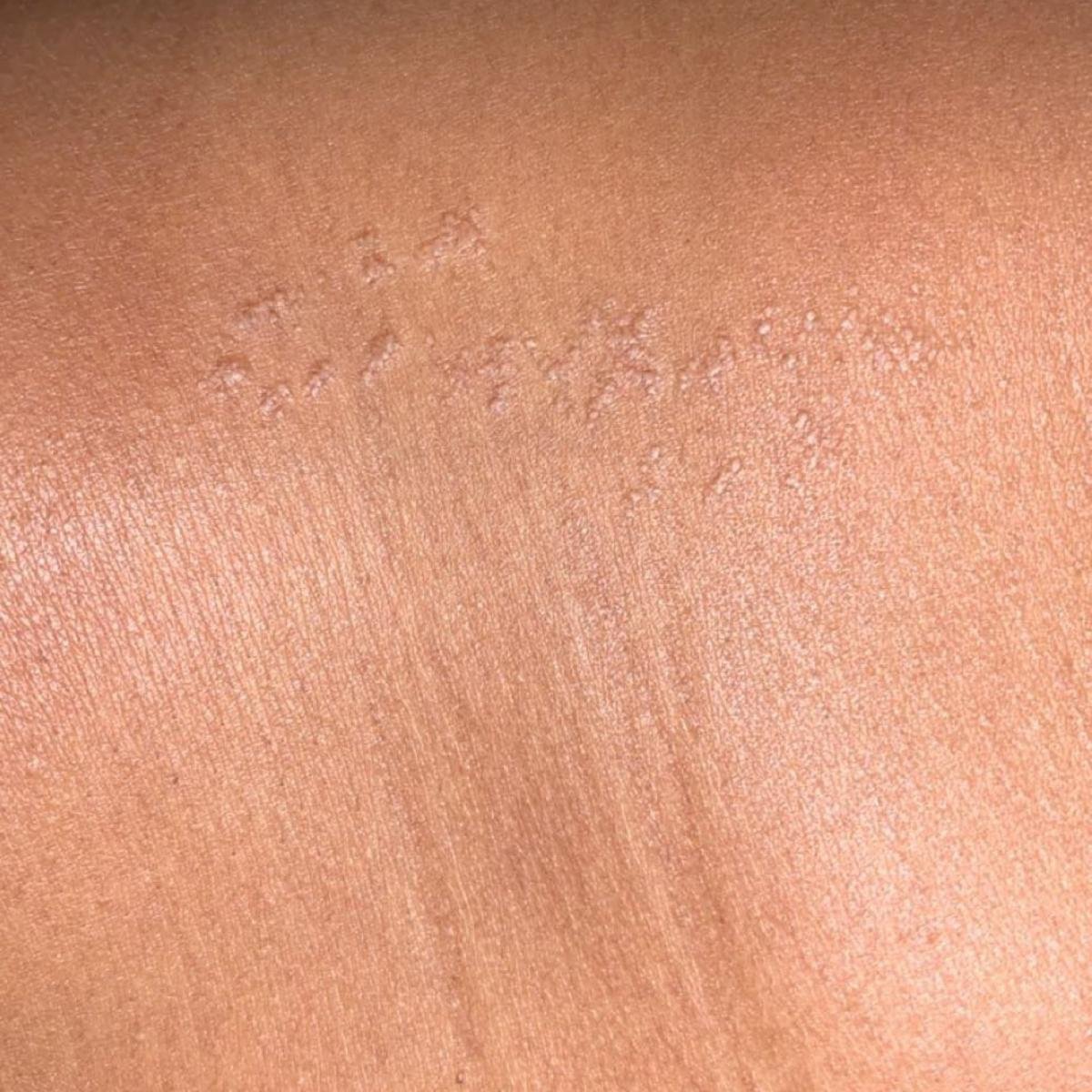
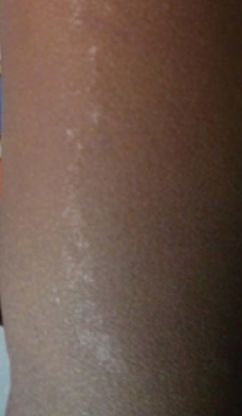
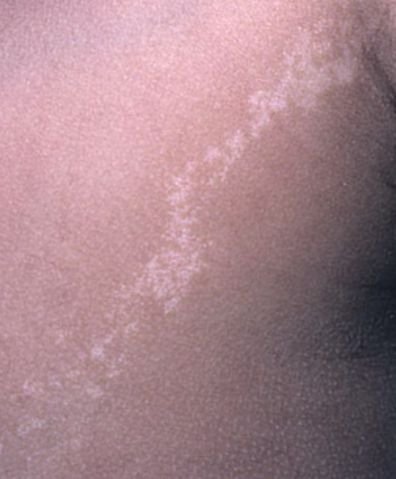
The hallmark sign of linear lichen is the appearance of small, flesh-colored to pink-red papules with a flat, scaly surface. These lesions usually arise linearly and follow Blaschko’s lines.
The rash is typically asymptomatic but may be accompanied by discomfort or visible cosmetic defects in extensive cases. Disease duration ranges from 3 to 12 months, and spontaneous remission is common. A residual post-inflammatory hyperpigmented linear streak may remain, fading within 3–4 years in most patients.
The diagnosis is usually based on clinical evaluation and patient history. The distinct linear pattern and typical distribution often suggest the diagnosis.
Linear lichen is typically a self-resolving condition. Treatment is not necessary in the majority of cases. However, in patients with significant itching or discomfort, symptomatic relief may be provided.
Linear lichen has a favorable prognosis. In the vast majority of cases, the condition resolves without complications within 12 months. Residual hyperpigmentation may persist for several years but tends to fade over time. Rarely, the pigment streak may remain lifelong, especially if the lichen was extensive or prolonged.
Psychological discomfort may occur in children or adolescents due to visible lesions, especially in exposed areas. However, relapses are extremely rare.
Linear lichen is a rare, benign, self-limiting inflammatory skin condition that presents in a distinct linear pattern and primarily affects children and adolescents. While its cause is not fully understood, it is not dangerous or contagious. Diagnosis is clinical in most cases, and treatment is usually unnecessary unless symptoms interfere with quality of life. Early consultation with a dermatologist ensures exclusion of other similar-appearing dermatoses and enables personalized skin care if needed.