Melanoma is a serious and extremely aggressive type of malignant tumor that originates in specialized skin cells known as melanocytes. These cells are responsible for the production of melanin—the natural pigment that determines the color of our skin, eyes, and hair. Unlike some other skin-related cells, melanocytes are not confined to the surface of the skin. They are also found in deeper anatomical regions, including mucous membranes (such as those in the mouth, nasal passages, and genitals) as well as the retina of the eye. Because of this widespread distribution, melanoma can develop in various locations across the body. This includes not only the skin but also internal surfaces such as the eyes, the genital area, the rectum, and even soft connective tissues. However, the vast majority—about 95%—of all diagnosed melanoma cases are found on the skin, making cutaneous melanoma the most prevalent form of the disease.
The dangerous reputation of melanoma comes from its unique biological behavior. Unlike many other skin tumors, melanoma is known for its ability to relapse repeatedly and to spread—often rapidly—to distant organs in the body. This metastatic spread, or metastasis, means that melanoma can move far beyond its original site and invade critical systems such as the lungs, liver, brain, and bones. Melanoma cells can migrate through the lymphatic system (lymphogenous route) or via the bloodstream (hematogenous route), further increasing the potential for widespread dissemination. One of the key factors influencing the speed and severity of melanoma progression is the state of the body’s immune system, particularly its innate ability to recognize and destroy abnormal or cancerous cells. When this natural antitumor defense is compromised, melanoma may advance at a much faster pace, making early detection and intervention crucial.
There are several clinically recognized types of melanoma, each with its own unique characteristics, prevalence, and typical outcomes. Understanding these subtypes helps in assessing prognosis and guiding treatment decisions:
Melanoma is most frequently diagnosed in individuals during their middle-aged years, typically between the ages of 30 and 50. This age range is considered the period of highest vulnerability due to cumulative sun exposure and gradual cellular changes that occur over time. While it is not impossible for melanoma to occur in younger individuals, such cases are exceedingly rare and often associated with strong genetic predispositions or congenital factors. In contrast, older adults—particularly those above 60 years of age—are more likely to develop what are known as lentiginous forms of melanoma. These forms are often linked to long-term sun damage and appear against a background of age-related pigmentation disorders such as lentigo or melanosis, especially on areas of the body that have been chronically exposed to the sun, like the face and forearms.
The transformation of normal melanocytes into malignant melanoma cells is a complex biological process influenced by a wide array of internal and external factors. These factors act either individually or in combination, gradually damaging the DNA within melanocytes and disrupting normal cellular behavior. Over time, these altered cells may acquire the ability to multiply uncontrollably, evade the immune system, and invade surrounding tissues, eventually developing into melanoma.
Although it is difficult to pinpoint a single, universal cause for melanoma, medical research has identified several contributing elements that are known to significantly increase the risk of its development. These risk factors do not act equally in all individuals, and the presence of one or more of them does not guarantee that melanoma will develop. However, their influence is substantial enough to warrant careful monitoring and preventive measures:
While the presence of these risk factors does not automatically mean that melanoma will develop, awareness and preventive strategies, including regular skin checks and protective measures against UV exposure, can dramatically reduce the chances of malignancy.
Diagnosing melanoma is a multi-step process that requires the combination of clinical expertise, specialized imaging tools, and laboratory analysis. The initial stage of diagnosis begins with a comprehensive clinical examination performed by a healthcare professional, typically a dermatologist or oncologist. During this examination, the medical specialist conducts a careful visual inspection of the suspicious lesion, paying close attention to its shape, color, size, and texture, as well as any noticeable changes over time.
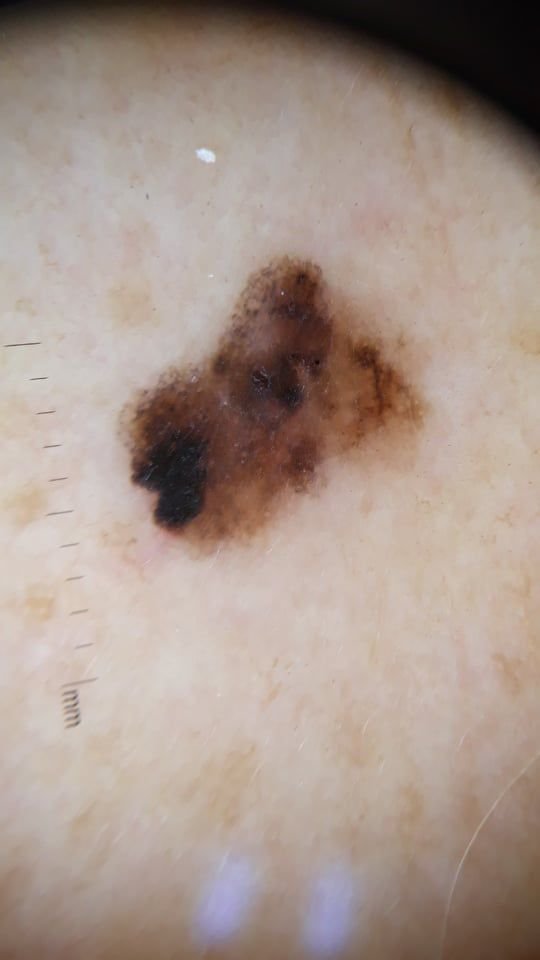
One of the key diagnostic tools used in this process is dermatoscopy (also known as dermatoscopy or epiluminescence microscopy). This non-invasive technique utilizes a handheld device with magnification and light to provide a detailed view of the internal structure of pigmented lesions. Dermatoscopy allows physicians to detect subtle patterns, irregularities, and abnormalities that may not be visible to the naked eye, significantly improving the accuracy of early melanoma detection.
However, while dermatoscopy offers important clues, it does not provide a definitive diagnosis. The only way to confirm whether a lesion is malignant melanoma is through histological examination, also known as a biopsy. In this procedure, the suspicious area—or the entire lesion—is surgically removed under local anesthesia and sent to a pathology laboratory. A pathologist then analyzes the tissue sample under a microscope to determine whether cancerous cells are present, their level of atypia, the depth of skin invasion, and other critical histological features. This microscopic analysis is considered the gold standard in melanoma diagnosis.
In cases where melanoma is confirmed, further diagnostic procedures are conducted to assess the extent of the disease. These include imaging tests such as ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) scans. These tests are used to examine regional lymph nodes and distant organs for signs of metastasis, which refers to the spread of cancer cells beyond the original site. Identifying whether metastases are present is crucial for determining the stage of melanoma and for guiding the appropriate course of treatment.
Overall, accurate and timely diagnosis is essential for improving outcomes in patients with melanoma. Early detection, supported by a combination of clinical evaluation, dermatoscopic imaging, and histopathological confirmation, remains the cornerstone of effective melanoma management and can significantly improve long-term survival rates.
The clinical presentation of melanoma varies widely, but there are hallmark visual signs that can alert both patients and medical professionals to its presence. A melanoma lesion may appear as a flat or raised spot, or a combination of both, on the surface of the skin. These lesions often exhibit a multiform appearance and tend to differ in texture, color, and shape from normal skin or benign moles. In the earliest stages—designated as stage 0 (in situ) or stage I—the natural skin pattern may still be preserved. However, as the disease progresses, the surface often becomes smooth, uneven, or nodular, with features like ulceration, crusting, and even spontaneous bleeding becoming apparent.
To standardize the early detection of melanoma, the medical community uses the widely accepted ABCDE system (introduced by Friedman in 1985), which is designed to help evaluate suspicious pigmented skin lesions:
Additional warning signs that may accompany or develop later include the disappearance of hair from within the mole, new sensations like tingling or burning, hardening of the lesion, the appearance of satellite spots around the main tumor, and the enlargement of nearby lymph nodes. If three or more of these symptoms appear simultaneously, the probability of melanoma is extremely high—over 80% according to clinical data.
While melanoma can appear anywhere on the body, there are some gender- and age-related patterns. Women are more likely to develop melanoma on the lower limbs (legs), while men most commonly exhibit it on the torso. In older adults, facial melanomas are more prevalent, often due to cumulative sun exposure over the years.
Dermatoscopy reveals highly specific visual patterns associated with melanoma, which can assist in distinguishing malignant lesions from benign ones. One of the key dermatoscopic findings is multicomponent structure—the presence of multiple overlapping visual characteristics within a single lesion.
Common dermatoscopic features of melanoma include:
It is critically important to distinguish melanoma from other pigmented or vascular skin lesions, as misdiagnosis can lead to delayed treatment and worse outcomes. Conditions that may resemble melanoma include:
Melanoma is widely recognized as one of the most aggressive and life-threatening types of skin cancer. Globally, the incidence of melanoma has been rising sharply, with the number of new cases doubling approximately every seven years. This alarming trend is primarily attributed to increasing exposure to ultraviolet (UV) radiation—both natural (from the sun) and artificial (from tanning beds)—and the tendency of people to travel more frequently to sunny regions, often without adequate sun protection.
Roughly half of all melanomas arise on skin that appears previously healthy, with no apparent pre-existing lesions. The remaining 50% emerge from previously benign pigmented neoplasms, such as moles. This dual origin complicates early detection and increases the risk of delayed diagnosis. While melanoma is about 10 times less common than other types of skin cancer (like basal or squamous cell carcinoma), it is responsible for the majority of skin cancer-related deaths. In fact, melanoma’s mortality rate is approximately 3.5 times higher than that of other malignant skin tumors.
When melanoma is suspected, it is crucial to consult a qualified oncologist or dermatologist without delay. The initial step involves thorough diagnostic evaluation, including clinical examination and biopsy. In cases where the diagnosis remains uncertain, a short-term observation period with frequent monitoring may be advised. However, more commonly, a complete excision of the suspicious lesion is performed, followed by histopathological analysis to confirm the diagnosis.
Once melanoma is confirmed, additional tests are carried out to determine whether the cancer has spread to nearby lymph nodes or distant organs. This staging process is essential for creating an individualized treatment plan and may involve imaging techniques such as CT scans, MRIs, or PET scans.
The cornerstone of melanoma treatment is surgical excision. Typically, this involves removing the tumor along with a margin of healthy skin to ensure complete eradication. The procedure is performed under local, regional, or general anesthesia depending on the tumor’s size and location. If the cancer has spread to regional lymph nodes, a lymphadenectomy (surgical removal of lymph nodes) may be required.
For patients with distant metastases, treatment becomes more complex and may involve a combination of chemotherapy, immunotherapy (including immune checkpoint inhibitors), targeted therapies based on genetic profiling of the tumor, and radiation therapy. Minimally invasive techniques or palliative surgery may also be used to relieve symptoms and improve quality of life.
It is important to note that superficial or minimally invasive procedures like laser therapy or cryodestruction are not considered adequate treatments for melanoma, even in its earliest stages. Such methods may leave malignant cells behind, leading to recurrence or metastasis.
Preventing melanoma begins with proactive and mindful care of the skin. Key preventive strategies include:
In addition, individuals with a personal or family history of melanoma, or those with multiple atypical moles, should consider periodic dermatoscopic monitoring. Early recognition and prompt removal of potentially dangerous lesions remains the most effective way to prevent the progression of melanoma to advanced stages.