Milium cyst, commonly referred to as “milia” or “milk spots,” is a small, white to yellowish, dome-shaped skin cyst that forms in the upper layers of the epidermis. These lesions are the result of the accumulation of keratin—a protein produced by skin cells—trapped beneath the surface of the skin. Unlike closed comedones, which form due to blockage of the sebaceous glands and hair follicles, milia are not associated with follicular structures or sebum obstruction.
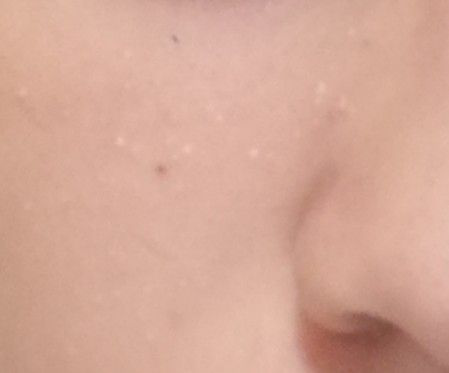
While milia are generally benign and painless, their appearance—particularly when clustered around the eyes, nose, or cheeks—can raise cosmetic concerns. They are most frequently seen on the face but can occur on any area of the body. Milium cysts can appear as single or multiple elements and are often mistaken for other types of cysts or acne lesions.
Milia are commonly observed in newborns as a physiological response to immature skin and disappear within a few months without intervention. However, a second peak of incidence is seen during adolescence and early adulthood, particularly in females. In adults, milia can appear spontaneously or be triggered by skin trauma, chronic irritation, or inappropriate cosmetic use. They may also be secondary to dermatoses or certain dermatological procedures such as laser resurfacing or dermabrasion.
The exact cause of milium cyst formation is multifactorial. The pathogenesis involves an imbalance in the processes of epidermal cell regeneration and exfoliation. Normally, keratinocytes (skin cells) are shed from the surface as part of the skin’s natural turnover. In milia, however, this process is impaired, leading to keratin entrapment beneath the stratum corneum. The build-up of keratin is then enclosed by a fibrous capsule, forming a distinct, superficial cyst.
While genetic predisposition is considered a primary factor, the condition may also be influenced or triggered by several internal and external conditions:
Although heredity plays a foundational role, these environmental and lifestyle factors can independently initiate or aggravate the pathogenesis of milia by disrupting the epidermal barrier and its regenerative functions. Addressing these triggers is vital to both treatment and long-term prevention.
The diagnosis of milium cysts is typically made during a clinical examination. A trained dermatologist can usually identify milia based on their distinct visual characteristics and anatomical location. Medical history is also important to determine whether the milia are primary (spontaneous, often congenital or idiopathic) or secondary (associated with skin trauma, underlying disease, or medical procedures).
In uncertain cases or when the lesions appear atypical, additional diagnostic steps may be warranted:
Proper diagnosis is essential not only to rule out similar-appearing lesions but also to determine the best course of treatment and identify underlying systemic factors if present.
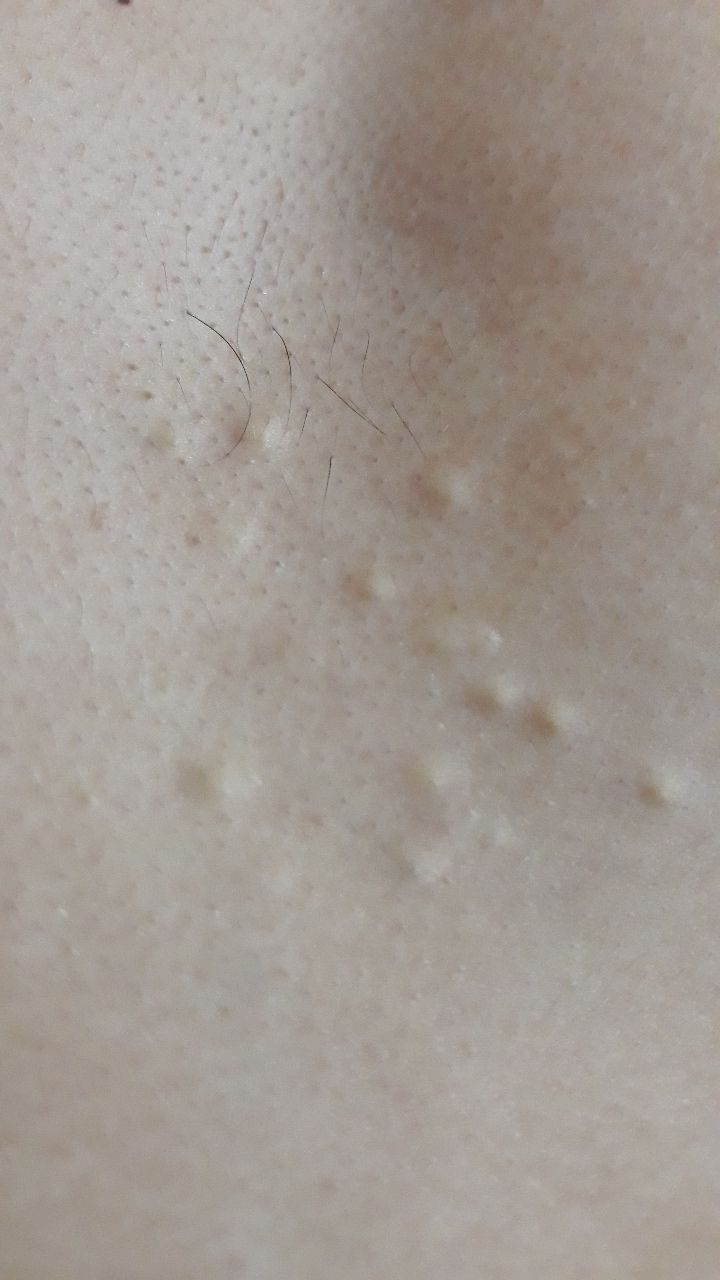
Milium cysts are typically small, white or yellowish papules that measure about 1–2 mm in diameter. They are well-circumscribed, firm, and dome-shaped, and they protrude slightly above the skin’s surface. Milia are most commonly located on the face—particularly around the eyes (periorbital region), nose, chin, forehead, and cheeks—but may also appear on the upper torso or genital region.
Clinical characteristics include:
In some cases, particularly with multiple lesions, milia may cover several square centimeters of skin. However, even in such presentations, the lesions remain isolated and do not coalesce.
Dermatoscopy enhances visualization and supports differential diagnosis. Typical dermatoscopic features of milium cysts include:
These dermatoscopic characteristics help distinguish milia from comedones, molluscum contagiosum, or other cystic and nodular lesions.
Although milia have a characteristic appearance, several other dermatologic conditions may resemble them. Differential diagnosis includes:
Although milium cysts are benign and non-life-threatening, their presence—especially in large numbers—can be indicative of underlying skin or systemic conditions, such as impaired epidermal turnover or endocrine imbalance. Milia serve as a visible sign that the skin’s natural renewal and shedding processes may be disrupted.
Risks associated with untreated or improperly treated milia include:
Although milia in newborns typically resolve on their own, persistent, multiple, or cosmetically concerning lesions in adolescents or adults should be evaluated by a dermatologist or cosmetologist. A professional consultation is essential when:
Close monitoring and individualized treatment help prevent recurrence, reduce cosmetic damage, and identify secondary causes that may otherwise go unnoticed.
Since milium cysts are located just below the epidermal surface, topical creams and over-the-counter treatments are generally ineffective. Self-removal is not recommended due to the risk of skin trauma, infection, and scarring.
Professional treatment options include:
After removal, it is essential to maintain proper skincare and implement preventive strategies to avoid the formation of new lesions.
Although not all cases of milia can be prevented, the risk of recurrence can be reduced through consistent skin care and healthy lifestyle habits:
With proper diagnosis, individualized treatment, and long-term preventive care, milium cysts can be effectively managed—restoring both the appearance and health of the skin.