Pityriasis Versicolor: Chronic Superficial Fungal Skin Infection
Overview
Pityriasis versicolor, also known as tinea versicolor, is a chronic, recurrent superficial fungal infection of the skin caused by yeast-like fungi of the genus Malassezia, most commonly Malassezia furfur. These lipophilic organisms are part of the normal skin flora, especially in sebaceous (oil-rich) areas. The infection results from the transformation of Malassezia from its commensal yeast form to a pathogenic mycelial form.
The condition is characterized by the presence of hypo- or hyperpigmented scaly macules and patches, often seen on the trunk and upper limbs. It is generally asymptomatic, though mild itching may occur in some patients. While it is not considered dangerous, pityriasis versicolor often causes aesthetic and psychosocial distress, particularly due to its visibility on exposed skin areas.
Pathogenesis and Triggering Factors
The transformation of Malassezia from a nonpathogenic yeast into its filamentous, pathogenic form is triggered by various internal and environmental factors that disrupt skin homeostasis. These include:
- Hot and humid climate: Promotes excessive sweating and sebum production, creating an ideal environment for fungal overgrowth;
- Hyperhidrosis: Increased sweating, particularly in athletes or during seasonal changes;
- Hormonal factors: Use of oral contraceptives, hormonal fluctuations, or endocrine disorders (e.g., Cushing’s syndrome);
- Immunosuppression: Conditions such as HIV/AIDS, cancer, or prolonged corticosteroid use;
- Genetic predisposition: A familial tendency has been observed in some individuals;
- Malnutrition and poor hygiene: Impaired skin barrier function may facilitate fungal proliferation.
Once activated, the fungi penetrate the stratum corneum (outermost skin layer), producing azelaic acid and other dicarboxylic acids, which inhibit melanin synthesis and lead to post-inflammatory pigmentation changes.
Clinical Presentation
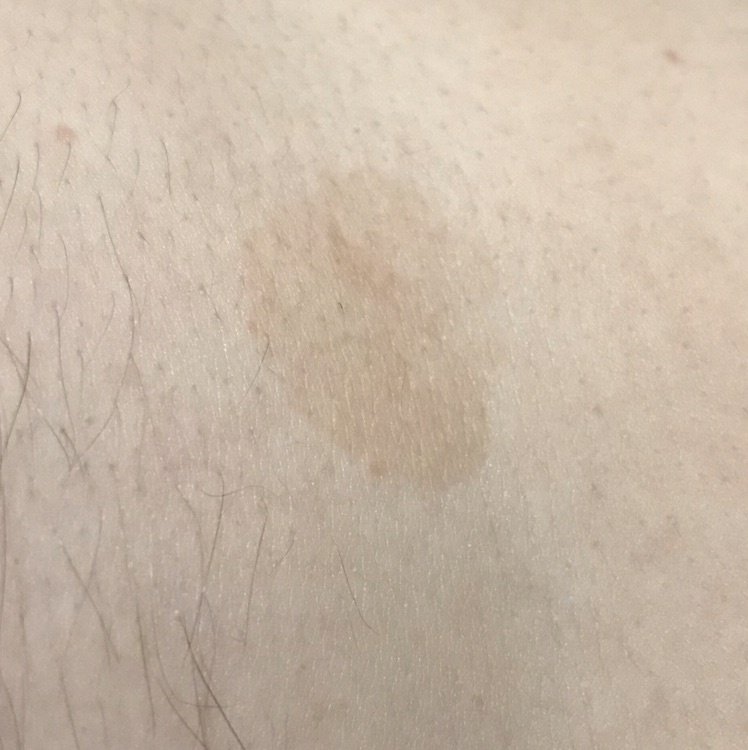
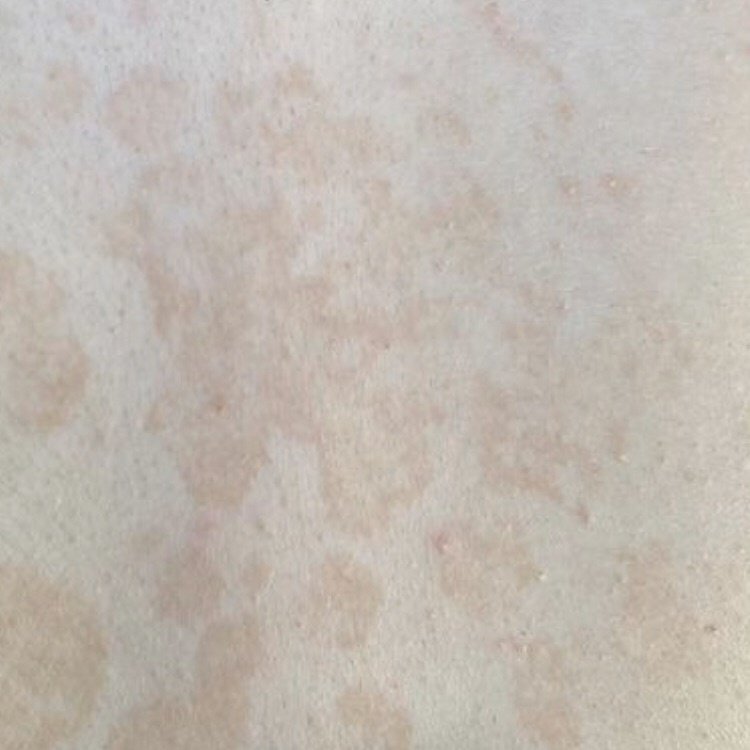
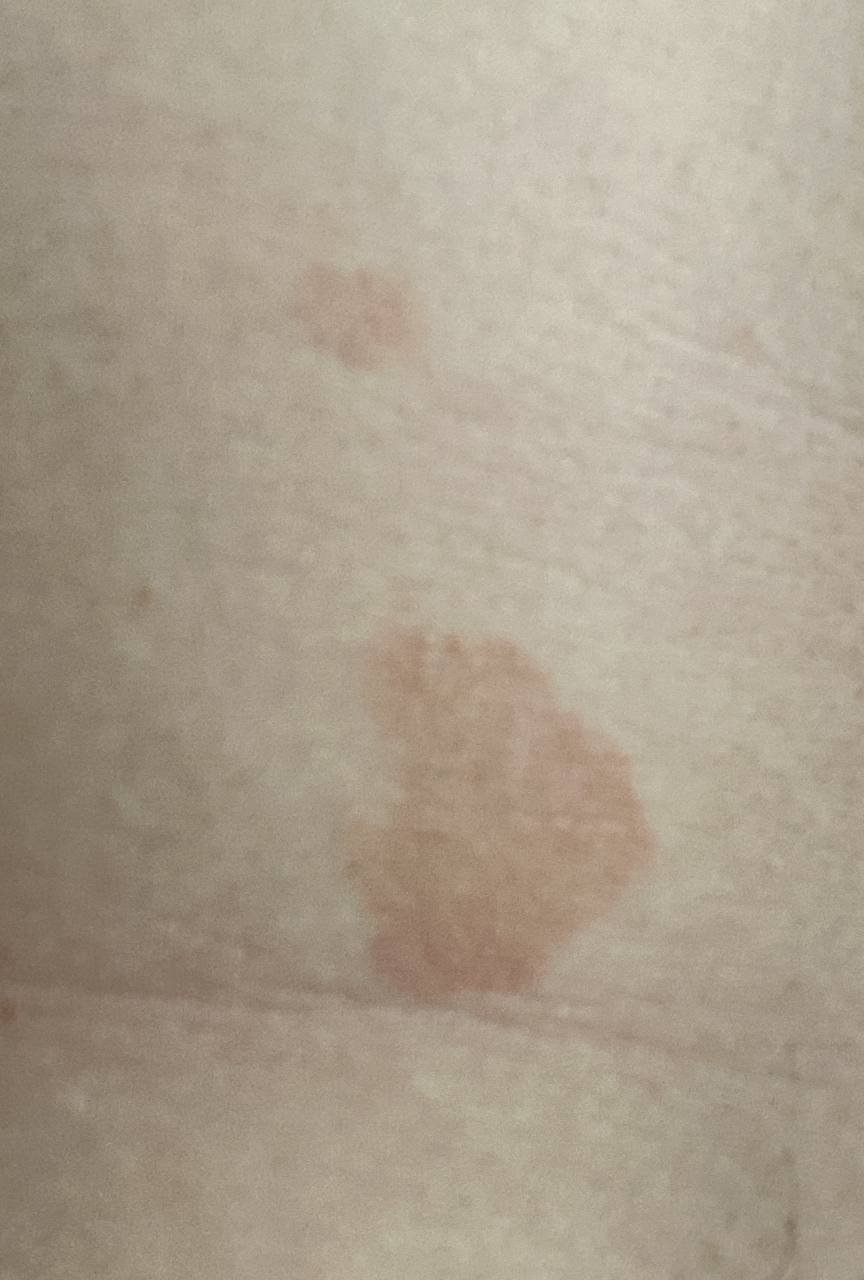
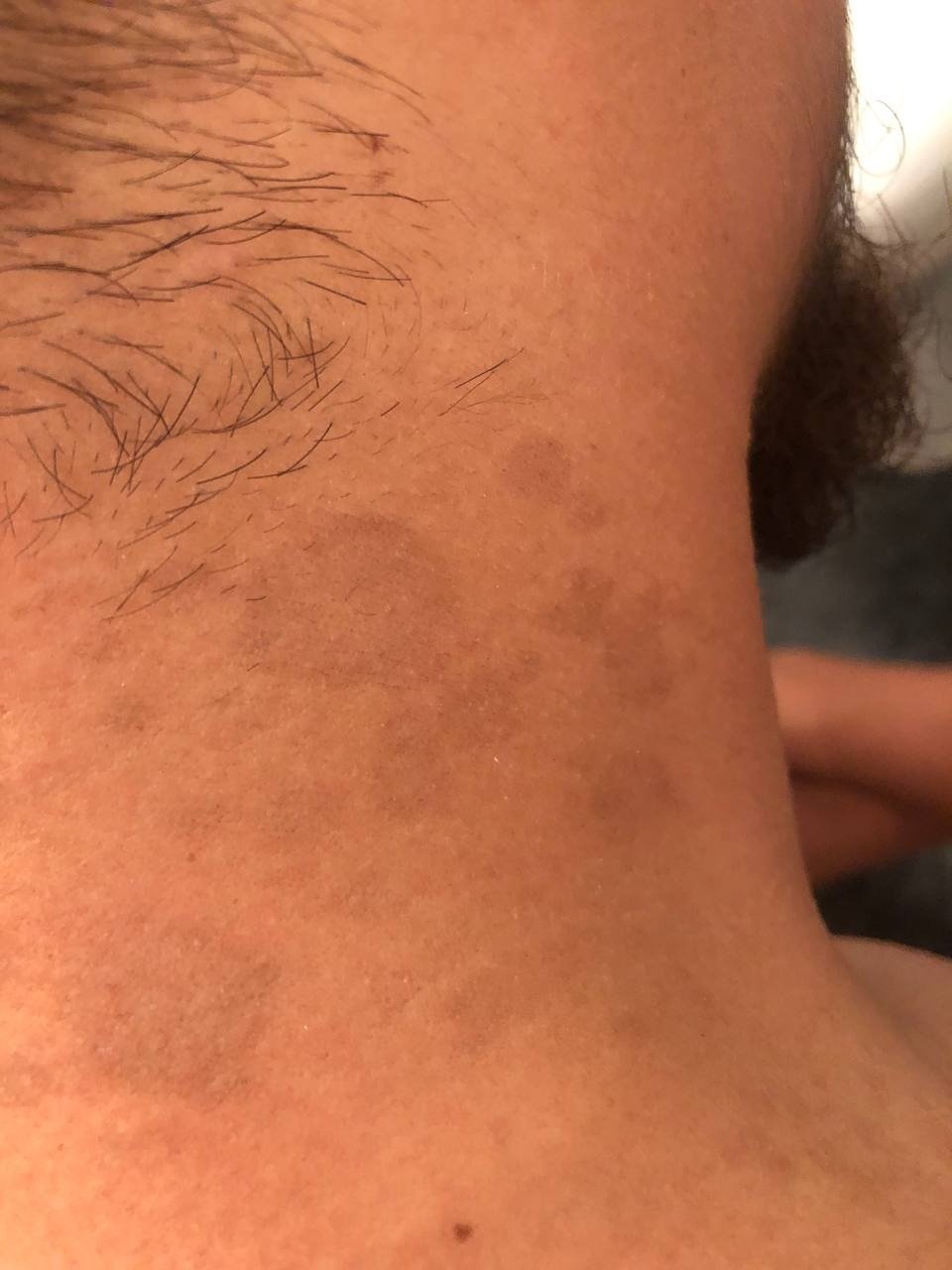
The hallmark of pityriasis versicolor is the development of well-demarcated, scaly, discolored patches that vary in hue—from pink, tan, and light brown to hypopigmented or chalky white, especially in darker-skinned individuals. In many cases, the lesions initially appear as small, round or oval spots up to 1 cm in diameter, but they often coalesce into larger patches over time.
Common characteristics include:
- Color: Varies depending on skin tone and stage of the lesion—“coffee with milk,” salmon-pink, yellow-brown, or lighter than surrounding skin;
- Scaling: Fine, bran-like scaling is typically visible when scratched (positive “scratch sign”);
- Borders: Sharply defined, may show centrifugal expansion;
- Symptoms: Generally asymptomatic or mildly itchy, especially when sweating increases.
Localization
Pityriasis versicolor predominantly affects sebaceous-rich and warm regions of the body. Typical areas of involvement include:
- Chest and upper back;
- Abdomen;
- Neck and shoulders;
- Proximal limbs (upper arms, thighs);
- Less frequently: Face, scalp, groin, and genital areas, usually in more extensive or recurrent cases.
After sun exposure, temporary hypopigmentation of previously affected skin areas may persist, leading to a mottled appearance known as “post-inflammatory leukoderma.” This effect is due to inhibition of melanogenesis and is reversible with time and treatment.
Follicular Variant of Pityriasis Versicolor
In addition to the classic macular form, pityriasis versicolor can also present in a follicular form, which is less common and may resemble bacterial folliculitis.
Key features of this variant include:
- Location: Commonly affects the chest, back, shoulders, and, occasionally, upper arms and thighs;
- Lesions: Multiple, small, red or flesh-colored papules or pustules centered around hair follicles (perifollicular distribution);
- Symptoms: May include itching, burning, or irritation—more intense than the classic macular form;
- Differential diagnosis: Required to distinguish from bacterial folliculitis—only direct microscopy or culture confirms the fungal etiology.
Diagnosis of Pityriasis Versicolor
Diagnosis is usually clinical and supported by simple, rapid laboratory techniques to confirm the fungal nature of lesions:
- Wood’s lamp examination: Lesions fluoresce a yellow-golden or orange glow under ultraviolet light, especially when caused by Malassezia furfur;
- Microscopic examination (KOH preparation): A skin scraping treated with potassium hydroxide reveals a characteristic “spaghetti and meatballs” appearance: short, curved hyphae and round spores;
- Culture: Creamy, mucilaginous colonies may grow on specialized lipid-enriched media, though cultures are rarely required for routine cases;
- PCR diagnostics: May be used in difficult or recurrent cases to identify Malassezia species at the molecular level.
Treatment of Pityriasis Versicolor
Therapeutic approaches depend on the severity, extent, and recurrence pattern of the infection. Both topical and systemic antifungal agents are effective, with topical treatment preferred for localized disease.
Topical Therapy (First-line for Mild to Moderate Cases):
- Ketoconazole 2% shampoo or cream: Applied once or twice daily for 2–4 weeks;
- Clotrimazole, terbinafine, or miconazole: Antifungal creams applied twice daily until clinical resolution;
- Selenium sulfide 2.5% lotion: Applied to the affected area and rinsed off after 10 minutes (used every other day);
- Zinc pyrithione or sulfur-based soaps: Used as maintenance or prophylaxis in recurrent cases.
Systemic Therapy (Moderate to Severe or Recurrent Cases):
- Itraconazole: 100 mg twice daily for 7–14 days;
- Fluconazole: 150–300 mg once weekly for 2–4 weeks (alternative regimen: 50 mg daily for 2 weeks);
- Ketoconazole (oral): 200 mg twice daily for up to 14 days (less favored due to hepatotoxicity risk; requires liver monitoring).
In all cases, patient adherence to treatment duration and hygiene recommendations is essential to prevent recurrence. In long-standing or extensive cases, a combination of oral and topical agents may be used.
Prevention of Pityriasis Versicolor
Because this condition has a high recurrence rate (especially in warm climates or predisposed individuals), preventive measures are important:
- Regular use of antifungal shampoos: Such as ketoconazole or selenium sulfide once or twice a week, especially during hot months;
- Proper skin hygiene: Shower daily, avoid tight clothing, and change sweat-soaked clothes promptly;
- Control of sweating: Use antiperspirants and wear breathable fabrics to reduce skin moisture;
- Limit prolonged sun exposure: Especially when recovering from recent outbreaks to avoid residual hypopigmentation becoming more visible;
- Manage underlying conditions: Such as immunodeficiency, malnutrition, or hormonal imbalances, when present.
Conclusion
Pityriasis versicolor is a common, superficial fungal infection caused by the overgrowth of Malassezia species on the skin. Although medically benign, its appearance and recurrence can cause significant cosmetic concern. Timely diagnosis, appropriate treatment, and long-term preventive strategies are essential to ensure sustained clearance and minimize relapse.
Through a combination of topical and systemic therapy, hygiene measures, and environmental control, most patients experience good outcomes. Education on recurrence patterns and maintenance options plays a critical role in effective management.