Pustular Psoriasis: Severe Variant of Chronic Psoriatic Dermatosis
Overview
Pustular psoriasis is a rare and severe form of psoriasis, characterized by the presence of sterile pustules on an erythematous, inflamed background. It can be localized or generalized and is considered by some dermatological schools as a distinct entity due to its distinct clinical behavior, prognosis, and management. Compared to plaque-type psoriasis, pustular psoriasis presents with a more aggressive course and may be associated with systemic symptoms and life-threatening complications.
This condition involves exaggerated immune-mediated inflammation and keratinocyte hyperproliferation, leading to epidermal dysfunction and pustule formation. It can affect both children and adults and may appear de novo or evolve from pre-existing psoriasis vulgaris.
Classification of Pustular Psoriasis
- Generalized pustular psoriasis (von Zumbusch type): Acute, life-threatening variant with systemic toxicity;
- Palmoplantar pustular psoriasis (Barber type): Chronic form affecting the palms and soles with painful sterile pustules;
- Annular pustular psoriasis: Ring-shaped lesions with pustules at the periphery, typically in children or during recovery;
- Acrodermatitis continua of Hallopeau: Involves distal digits, leading to nail loss and bone involvement in long-term disease;
- Impetigo herpetiformis: A rare, potentially fatal form of pustular psoriasis occurring in pregnancy, associated with hypocalcemia and fetal risks.
Etiology and Triggering Factors
The precise etiology of pustular psoriasis remains unclear. It is believed to involve a genetically predisposed immune dysregulation, often exacerbated by external or internal triggers. Unlike psoriasis vulgaris, known associations with the HLA-Cw6 gene are less prominent.
Potential triggers include:
- Medications: Sudden withdrawal of systemic corticosteroids, antimalarials, beta-blockers, lithium, NSAIDs, certain antibiotics (penicillin), oral contraceptives, or calcipotriol;
- Infections and systemic diseases: Bacterial, viral infections, or underlying immunosuppression;
- Physical or chemical irritants: Chemical exposure, trauma, burns, or strong irritant contact;
- Hormonal changes: Pregnancy or menopause;
- Psychological stress;
- Smoking and excessive UV exposure;
- Pre-existing psoriasis vulgaris: May evolve into pustular form under stressors listed above.
Clinical Presentation
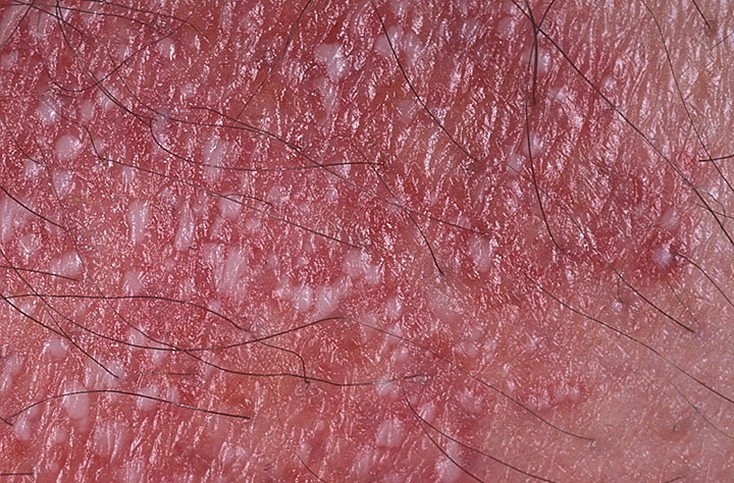
Pustular psoriasis presents with superficial sterile pustules that can be widespread or localized, often associated with fever, malaise, and systemic toxicity in generalized forms. These pustules contain neutrophilic exudate and are not infectious.
Skin findings include:
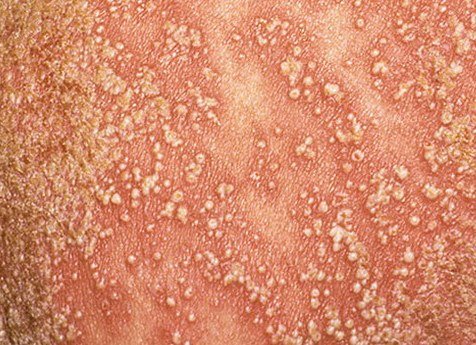
- Pustules: Raised, non-follicular vesicles filled with yellowish fluid, appearing on inflamed, red skin;
- Surrounding erythema: Bright red, warm, swollen, and exfoliative plaques around and beneath pustules;
- Peeling and desquamation: Following pustule rupture, large sheets of skin may shed;
- Common locations: Palms and soles (localized type), limbs, trunk (generalized type);
- Systemic symptoms: Chills, fatigue, arthralgia, fever, dehydration in severe forms;
- Secondary bacterial infection: May occur if pustules rupture and skin barrier is compromised.
Course: Chronic with flares, or acute life-threatening exacerbations requiring hospitalization. Without proper intervention, generalized forms can lead to serious complications and mortality.
Diagnostics
Diagnosis of pustular psoriasis is primarily clinical and based on history and the appearance of pustular lesions on erythematous skin. The presence of typical psoriatic plaques and systemic symptoms supports the diagnosis. Diagnostic steps include:
- Physical examination: Identifying sterile pustules, distribution pattern, systemic symptoms, and history of psoriasis;
- Auspitz triad (in some cases):
- Stearin spot phenomenon: Easy removal of scales from plaques;
- Terminal membrane: Smooth red film under the scale;
- Point bleeding: After scratching, small pinpoint hemorrhages appear.
- Skin biopsy: Performed in uncertain cases. Histology reveals spongiform pustules of Kogoj, acanthosis, and Munro microabscesses;
- Culture of pustular contents: To exclude bacterial infection;
- Blood tests: Check for anemia, elevated inflammatory markers (ESR, CRP), electrolyte imbalances, and liver/kidney function.
Differential Diagnosis
Pustular psoriasis must be differentiated from other pustular and scaly dermatoses, including:
- Dermatophyte infections: Especially tinea of hands and feet;
- Dyshidrotic eczema: Vesicles with clear fluid, pruritus, often bilateral;
- Keratoderma blennorrhagicum: Seen in reactive arthritis, affecting palms/soles;
- Impetigo and pyoderma: Bacterial infection with purulent pustules;
- Toxicoderma: Drug-induced pustular eruptions;
- Generalized pustulosis of pregnancy (impetigo herpetiformis): A severe form during pregnancy.
Treatment
The goal of treatment is to reduce pustule formation, inflammation, and keratinocyte proliferation, and to manage systemic symptoms. Treatment is individualized based on severity and comorbidities.
Topical therapy:
- Keratolytic agents: Urea, salicylic acid to reduce scale and soften plaques;
- Topical corticosteroids: Mid- to high-potency agents to reduce inflammation;
- Calcineurin inhibitors: Tacrolimus for sensitive areas (off-label);
- Topical retinoids: In selected cases (e.g., tazarotene);
- Emollients: Used daily to restore barrier function and comfort.
Systemic therapy:
Indicated in:
- Generalized pustular psoriasis;
- Psoriatic arthritis;
- Failure of topical or phototherapy.
- Oral retinoids: Acitretin is commonly used, particularly in pustular variants;
- Immunosuppressants: Methotrexate, cyclosporine in severe or recalcitrant cases;
- Biologic agents: TNF-α inhibitors (adalimumab), IL-17 inhibitors (secukinumab), IL-12/23 inhibitors (ustekinumab), and PDE-4 inhibitors (apremilast);
- Systemic corticosteroids: Generally avoided due to risk of rebound flare on withdrawal, but may be used in life-threatening situations under supervision;
- Phototherapy: UVB or PUVA therapy may be used in stable disease, but is typically avoided in active pustulosis.
Complications
Compared to plaque psoriasis, pustular psoriasis is associated with more serious and potentially life-threatening complications, particularly in generalized forms:
- Secondary infections (pyoderma): From ruptured pustules;
- Alopecia and onycholysis: Hair loss and nail destruction;
- Metabolic disturbances: Hypoalbuminemia, hypocalcemia;
- Organ damage: Renal failure (due to acute tubular necrosis), liver failure in systemic involvement;
- Sepsis and multi-organ failure: Seen in untreated or fulminant generalized pustular cases;
- Mortality risk: Estimated at 2% in severe, untreated cases with complications.
Prevention
Although pustular psoriasis is not always preventable, the frequency and severity of flares can be reduced by:
- Avoiding trigger medications: Never discontinue corticosteroids abruptly; avoid self-medication with NSAIDs, antibiotics, or hormonal drugs without medical advice;
- Managing stress: Psychological support or therapy for stress-induced flares;
- Maintaining skin barrier function: Daily use of moisturizers, avoidance of irritants;
- Smoking cessation and alcohol moderation;
- Healthy lifestyle: Balanced diet, regular physical activity, management of metabolic comorbidities (e.g., diabetes, obesity);
- Close monitoring: Regular follow-up with dermatology and lab evaluation during systemic therapy.
Conclusion
Pustular psoriasis is a severe inflammatory skin disease that may present as a localized or generalized condition. It requires early diagnosis and aggressive management to prevent complications. With advances in topical, systemic, and biologic therapies, most patients can achieve significant symptom relief and disease control. Interdisciplinary care, patient education, and adherence to therapy are essential for long-term success and improved quality of life.