Ring-shaped Centrifugal Erythema (RCE), also known as erythema annulare, is a dermatological condition characterized by ring-like rashes on the skin, resembling urticaria. These papules expand outward from a central area, forming a distinct circular pattern. RCE is classified as a form of erythema annulare and typically occurs in response to an allergenic or infectious trigger, although in some cases, no specific cause is identified.
RCE was first described in 1916 by French dermatologist Ferdinand-Jean Darier, who recognized its characteristic circular lesions and distinct clinical features.
RCE is considered a type of reactive erythema, a condition in which the skin reacts to external triggers. Although the precise causes of RCE are not fully understood, the condition is often associated with infections, medications, chemicals, or malignancies (paraneoplastic syndrome). In some cases, the condition occurs without any identifiable trigger, in which case it is referred to as the idiopathic form.
From a histological perspective, RCE typically involves intense lymphohistiocytic infiltration around dermal vessels. The epidermis remains unaffected, making it a primarily dermal condition.
RCE is considered a relatively rare condition, with an annual incidence of approximately 1 case per 100,000 people. It affects all sexes and races equally, with the peak onset occurring around the age of 40. A rare autosomal dominant form of RCE, known as familial ring-shaped erythema, has also been documented, indicating a genetic component in some cases.
RCE is classified as a type IV hypersensitivity reaction. Several triggers have been identified, including:
RCE lesions may also arise in response to autoimmune diseases, stress, hormonal changes, and dietary factors like moldy cheeses and tomatoes.
RCE is often triggered by various infections, including:
Medications, such as amitriptyline, chloroquine, and azacitidine, have been found to trigger RCE in some individuals. RCE symptoms typically resolve once the causative medication is discontinued.
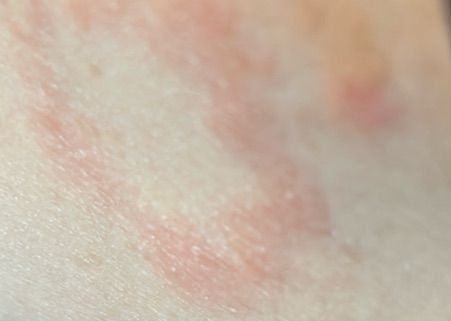
Patients with RCE typically present with ring-shaped erythematous papules that begin as small, red spots in the center and expand outward. These lesions often appear on the thighs, shins, and occasionally on the trunk and face. The skin changes may accompany systemic symptoms, such as fever and night sweats, particularly in cases related to tuberculosis or lymphoma.
Typically, lesions start as erythematous papules that enlarge peripherally and clear centrally, forming a ring-like appearance. These lesions may exceed 10 cm in diameter. In many cases, scaling is seen along the outer edge, and vesicles or telangiectasias may appear. When the lesions resolve, they often leave behind post-inflammatory hyperpigmentation, but without scarring.
Patients may experience either asymptomatic or itchy rashes, depending on the allergen or trigger. Some lesions may be painful, especially in cases involving systemic diseases or infections.
RCE generally has a favorable prognosis, especially when the underlying cause is identified and treated promptly. However, the prognosis may worsen in patients with concurrent systemic or malignant conditions. The duration of the lesions can vary, with some cases resolving within weeks, while others may persist for several years.
According to Ackerman, and later Bressler and Jones, RCE has two clinical forms:
Diagnosing RCE involves a thorough medical history review, physical examination, and laboratory testing if necessary. If malignancy is suspected, patients should undergo appropriate oncological screening.
Diagnostic methods include:
RCE must be distinguished from various other dermatological conditions that present with similar symptoms, including:
It is also important to differentiate RCE from other similar conditions like:
Treatment for RCE focuses on addressing the underlying cause of the condition. Once the trigger is identified and treated, the skin lesions often resolve on their own. For idiopathic cases or when the cause remains unclear, symptomatic treatments may include:
Long-term follow-up is essential as relapses can occur after treatment cessation. A dermatologist should guide therapy, particularly for recurrent or severe cases of RCE.
To prevent flare-ups of RCE, individuals should avoid known triggers and take proactive steps to maintain skin health: