Rosacea is a chronic, progressive inflammatory dermatosis that primarily affects the central region of the face. It is associated with hyperreactivity of cutaneous blood vessels, disruption in the regulation of microcirculation, and secondary involvement of the sebaceous glands and hair follicles. The clinical picture of rosacea varies widely, depending on the stage and subtype of the disease, but may include persistent erythema, flushing episodes, telangiectasia, papules, pustules, rhinophyma, and even ocular involvement.
Although rosacea may resemble acne vulgaris due to the presence of papulopustular lesions, it is an independent disease with a distinct etiology, pathogenesis, and therapeutic approach. The key distinguishing factor is its vascular origin and the characteristic central facial involvement in middle-aged adults. However, both conditions can coexist in the same patient, making accurate diagnosis and tailored treatment critical.
Rosacea typically manifests between the ages of 30 and 50 years, often with a gradual progression of symptoms. It is most common among individuals with fair skin (Fitzpatrick skin phototypes I–II), particularly those of Northern European descent. The global prevalence is estimated at around 10% of the adult population, although many cases remain underdiagnosed or misdiagnosed, especially in the early stages.
The pathogenesis of rosacea involves a complex interplay of neurovascular dysregulation, immune dysfunction, and changes in the skin’s microbiome. The initial trigger is often an abnormal dilation of facial capillaries in response to various stimuli such as heat, alcohol, spicy food, or stress. Repeated episodes of vasodilation result in persistent flushing and eventual structural changes to the vessel walls, which lose elasticity and lead to visible telangiectasias. Simultaneously, a dysregulated immune response promotes inflammation and the proliferation of Demodex folliculorum and other opportunistic microbes on the skin.
With progression, the skin’s barrier function deteriorates, contributing to increased transepidermal water loss, dryness, and hypersensitivity. Over time, this cascade of vascular and inflammatory events results in the development of fixed erythema, inflammatory papules, and in some patients, phymatous changes characterized by soft tissue hypertrophy and fibrosis.
While the precise cause of rosacea remains unclear, several risk factors and triggers have been identified that contribute to disease onset and exacerbation. These include:
Understanding and addressing these factors is essential for both prevention and management. While not all triggers are avoidable, minimizing exposure and strengthening the skin’s vascular and barrier functions can reduce disease activity and improve quality of life.
The diagnosis of rosacea is clinical and is based on a combination of medical history, symptom chronology, and a detailed dermatological examination. It is essential to distinguish rosacea from other dermatoses that may present with facial redness or pustular lesions, especially in early or atypical cases. A well-conducted anamnesis should include identifying triggers, the pattern of disease onset, flushing episodes, photosensitivity, and any previous skin treatments or comorbidities.
Diagnostic tools and procedures may include:
Rosacea presents in a spectrum of clinical subtypes, which may exist independently or overlap in the same patient. Understanding the clinical presentation is essential for subtype classification and treatment planning.
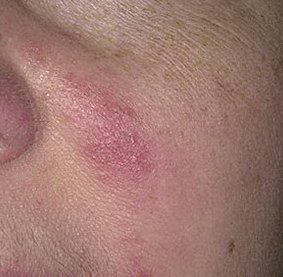
This early form of rosacea is characterized by episodic or persistent facial flushing (also known as “blushing”) that becomes more frequent and longer-lasting over time. Initially, flushing resolves completely but eventually results in persistent erythema and the appearance of fine, dilated blood vessels—telangiectasias. Skin may feel warm, sensitive, or experience mild stinging or itching. Over time, the erythema may deepen in color and occupy broader areas of the cheeks, nose, chin, and forehead.
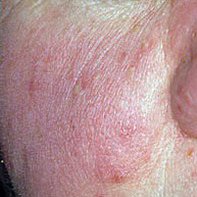
This stage develops on a background of erythema and is defined by the presence of papules (inflamed red bumps) and pustules (pus-filled lesions), often in symmetrical clusters on the central face. Unlike acne, these lesions are not accompanied by comedones. The skin appears inflamed, and the patient may experience increased skin sensitivity, dryness, and visible inflammation. In more severe cases, pustules may be numerous and confluent.
This subtype involves chronic inflammation and fibrosis leading to soft tissue hypertrophy, particularly of the nose, resulting in bulbous, lobulated contours and a purple-cyanotic hue. Phymatous changes can also affect the chin, forehead, and cheeks. The skin appears thickened, oily, with enlarged pores, and may contain visible nodules. Rhinophyma is more common in men and may require surgical correction.
Ophthalmic involvement occurs in up to 50% of patients and may precede cutaneous signs. Symptoms include burning, foreign body sensation, dryness, eyelid margin inflammation (blepharitis), and conjunctival redness. If untreated, ocular rosacea can lead to corneal involvement and visual impairment. Prompt referral to an ophthalmologist is crucial in such cases.
Rosacea must be differentiated from other conditions with overlapping symptoms:
Although rosacea is not life-threatening, its chronic, relapsing nature and progressive vascular damage can lead to significant disfigurement and psychosocial distress if left untreated. Patients often report embarrassment, reduced self-esteem, social anxiety, and even depression due to visible symptoms.
Additionally, rosacea may be a cutaneous marker of underlying systemic imbalances such as gastrointestinal dysbiosis, hormonal disturbances, or chronic inflammation. Ocular involvement presents a risk to vision, especially when corneal ulcers or blepharitis are inadequately managed.
Complications of untreated rosacea include:
Patients should consult a dermatologist as soon as signs of chronic facial redness, flushing, or papulopustular lesions develop. Early intervention can slow disease progression, reduce complications, and improve long-term outcomes.
Clinical management should include:
Effective rosacea treatment requires a stepwise, personalized approach, combining prescription medications, procedural therapies, and lifestyle adjustments. Key components include:
Consistency and adherence to the treatment regimen are critical. Patients should be educated about the chronic nature of rosacea and the importance of maintenance therapy even during remission periods.
Rosacea prevention involves not only skincare but also systemic health and lifestyle management. Key preventive strategies include:
With a proactive and informed approach—supported by qualified medical care—most individuals with rosacea can achieve stable remission, minimize flare-ups, and preserve both skin health and self-confidence.