Seborrheic Dermatitis: Chronic Inflammatory Skin Condition
Overview
Seborrheic dermatitis is a chronic inflammatory dermatosis that typically affects areas of the skin with a high density of sebaceous glands. It presents with symptoms such as redness, flaking, greasy scales, and mild pruritus. Though not contagious or dangerous, it often causes significant cosmetic concern and emotional discomfort, particularly when located on the face or scalp.
This condition affects both infants (cradle cap) and adults. While in infants it usually resolves on its own within a few months, in adults it tends to follow a relapsing-remitting course that may require periodic treatment.
Etiology and Risk Factors
The exact cause of seborrheic dermatitis is not fully understood, but it is believed to result from a combination of factors, including:
- Overgrowth of Malassezia yeast: Lipophilic fungi such as Malassezia furfur are part of the normal skin flora but may trigger inflammation when overgrown in sebaceous areas;
- Hormonal influence: In infants, maternal hormones transmitted before birth may play a role;
- Immune system dysfunction: More common in individuals with weakened immunity (e.g., HIV/AIDS, chemotherapy);
- Genetic predisposition: Family history of seborrheic dermatitis or similar skin conditions.
Triggering and exacerbating factors include:
- Cold and dry weather;
- Stress and psychological factors;
- Hormonal fluctuations (e.g., puberty, pregnancy);
- Harsh soaps, shampoos, and detergents;
- Underlying neurological or systemic diseases (e.g., Parkinson’s disease, epilepsy, depression);
- Alcohol consumption, poor nutrition, and certain medications.
Symptoms
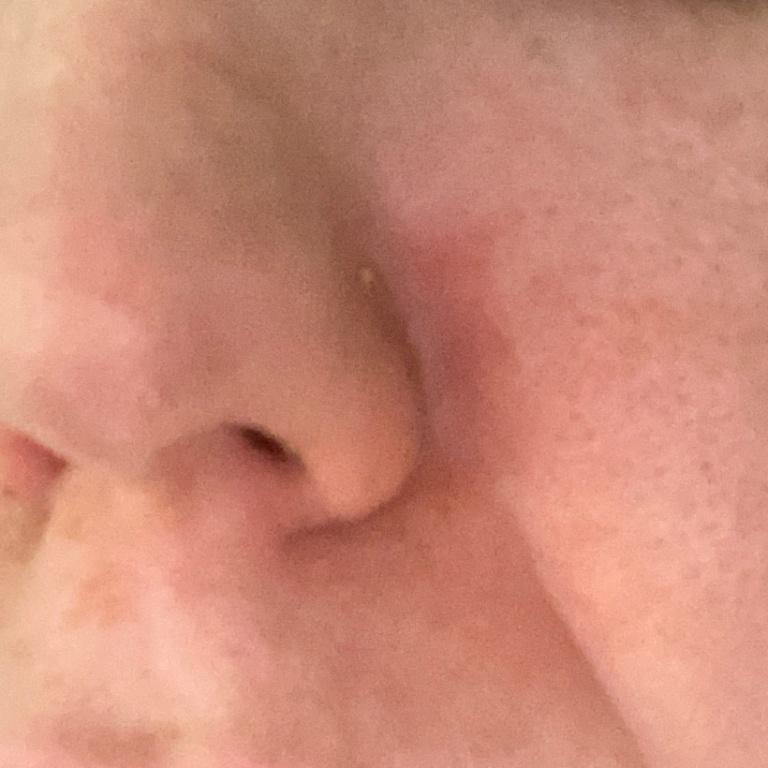
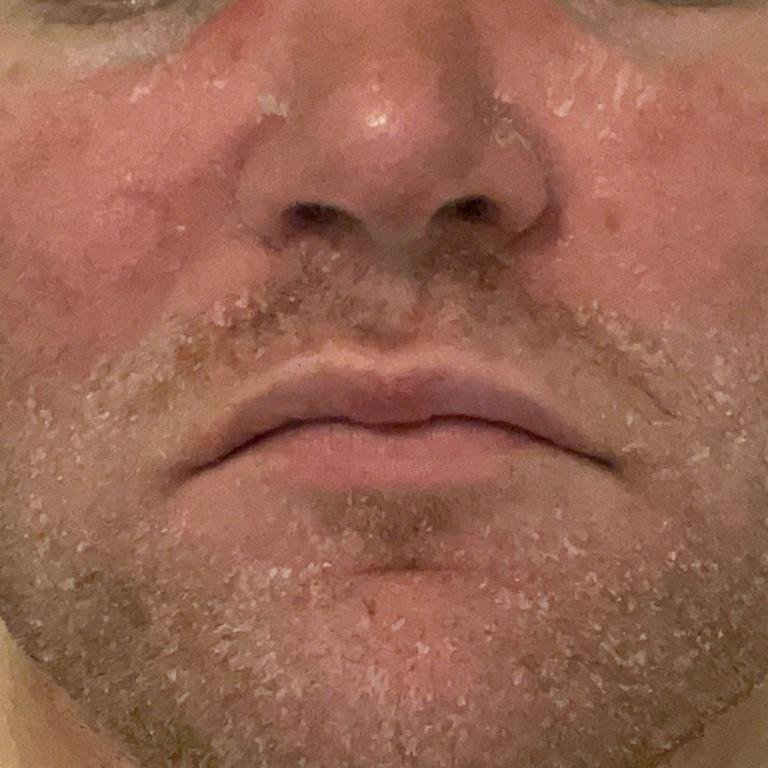
Seborrheic dermatitis may occur on any part of the body, but it primarily affects areas rich in sebaceous glands. The most common sites include:
- Scalp (dandruff or more inflamed scalp lesions);
- Eyebrows, eyelashes, and nasolabial folds;
- Behind the ears and external ear canal;
- Upper chest and back;
- Axillary and groin folds (in severe or generalized cases).
Typical clinical features include:
- Greasy, yellowish scales over erythematous (red) skin;
- Mild to moderate itching or burning sensation;
- Peeling and flaking (dandruff);
- Waxy skin texture, especially in areas with folds or behind the ears;
- In infants: thick crusts on the scalp (“cradle cap”), erythema, and flaking in the diaper area.
When to See a Doctor
Consultation with a dermatologist is advisable when:
- Symptoms persist despite proper skin care and over-the-counter products;
- There is significant redness, swelling, or signs of secondary bacterial infection (oozing, pus, pain);
- Lesions appear in unusual locations (e.g., eyelids, genitals), are rapidly spreading, or causing significant discomfort;
- Differential diagnosis is needed to rule out similar conditions, such as psoriasis, rosacea, contact dermatitis, or lupus erythematosus.
Complications
Complications of seborrheic dermatitis may include:
- Secondary bacterial infection: Especially in adults or immunocompromised patients; presents with increased pain, erythema, moisture, and crusting;
- Side effects of treatment: Prolonged use of topical corticosteroids can lead to skin atrophy, telangiectasia, and barrier dysfunction;
- Psychosocial impact: Visible lesions on the face or scalp may lead to anxiety, embarrassment, or decreased quality of life.
Diagnostics
The diagnosis of seborrheic dermatitis is usually based on clinical presentation and patient history. In most cases, no additional tests are required. However, diagnostic clarification may be necessary in atypical cases or when other conditions are suspected.
Diagnostic methods include:
- Physical examination: Evaluation of lesion distribution (scalp, nasolabial folds, chest) and morphology (greasy scales, erythema);
- Dermatoscopy: Helps assess scaling pattern, follicular involvement, and vascular features;
- Skin scrapings with KOH microscopy: Used to exclude dermatophyte or Candida infection in doubtful cases;
- Biopsy: Rarely needed. Histology may reveal parakeratosis, spongiosis, and mild perivascular infiltrates.
Treatment of Seborrheic Dermatitis
Treatment strategies depend on the severity, location, and chronicity of the disease. The goal is to reduce inflammation, control fungal overgrowth, and alleviate flaking and itching.
Topical treatment options:
- Antifungal agents: Ketoconazole, clotrimazole, ciclopirox (shampoos, creams); applied 1–2 times daily for 2–4 weeks;
- Topical corticosteroids: Low- or medium-potency steroids for limited flare-ups (e.g., hydrocortisone, desonide); avoid prolonged use due to risk of atrophy;
- Calcineurin inhibitors: Tacrolimus or pimecrolimus—useful on sensitive areas such as eyelids, face, and folds;
- Keratolytic agents: Salicylic acid, sulfur, or selenium sulfide shampoos help remove thick scales;
- Moisturizers: Regular use of emollients to maintain skin barrier function and reduce scaling.
Systemic therapy:
- Systemic antifungals: Itraconazole (100 mg BID) or fluconazole (50–100 mg daily) for widespread or refractory seborrheic dermatitis (prescribed under medical supervision);
- Short courses of oral corticosteroids: Occasionally used in severe flares with intense inflammation (rare and with caution).
Skincare Guidelines and Lifestyle Adjustments
Effective long-term control of seborrheic dermatitis includes gentle skin care and avoidance of known triggers:
- Daily cleansing: Use mild, fragrance-free cleansers or baby shampoos for facial skin and scalp;
- Scalp care: Brush off loose scales before shampooing; apply mineral or olive oil for 30–60 minutes before washing for thick crusts;
- Avoid harsh cosmetics: Steer clear of alcohol-based products, aggressive exfoliants, and strong soaps;
- Hair and facial product restriction: Avoid styling gels and sprays during active flare-ups;
- Manage stress: Psychological stress is a known exacerbator of seborrheic dermatitis;
- Wear breathable clothing: Cotton garments reduce irritation in affected skin folds.
Prevention
Although seborrheic dermatitis is not curable, recurrences can be minimized with consistent prevention:
- Maintain regular use of antifungal or medicated shampoos as maintenance (e.g., twice weekly);
- Avoid environmental extremes (cold, dry air) and known personal triggers;
- Moisturize regularly, especially in winter months or after bathing;
- Consult your dermatologist promptly when flare-ups occur or if new symptoms develop;
- Limit alcohol intake and optimize nutrition;
- In infants, avoid overheating, and cleanse gently with warm water and mild cleansers.
Conclusion
Seborrheic dermatitis is a common, chronic skin condition affecting sebaceous-rich areas of the body. While benign in nature, its visible manifestations and recurring nature can affect self-esteem, comfort, and quality of life. With proper diagnosis, targeted therapy, and maintenance care, most patients can achieve long-term symptom control and reduce flare frequency.
Dermatologic follow-up and individualized treatment plans are key to managing more persistent or severe forms, especially when seborrheic dermatitis overlaps with other skin conditions or systemic illnesses.