Seborrheic Keratosis is a benign skin tumor characterized by keratinization, which rises above the skin surface. These lesions typically appear after the age of 50, with their prevalence increasing with age. Seborrheic keratosis is commonly found in multiples, and the number of lesions tends to grow over time. This type of neoplasm is equally common in both men and women, although the frequency may vary slightly based on age and other factors.
The exact cause of seborrheic keratosis remains unclear, but several factors have been identified that may increase the risk of developing these benign skin lesions. These factors contribute to the appearance and growth of seborrheic keratosis:
The diagnosis of seborrheic keratosis is based on a clinical examination, which includes a routine visual inspection of the lesion and dermatoscopic evaluation to assess the characteristics of the growth. If there are concerns that the lesion may be malignant or atypical, a biopsy may be performed to confirm the diagnosis and exclude other conditions, such as skin cancer.
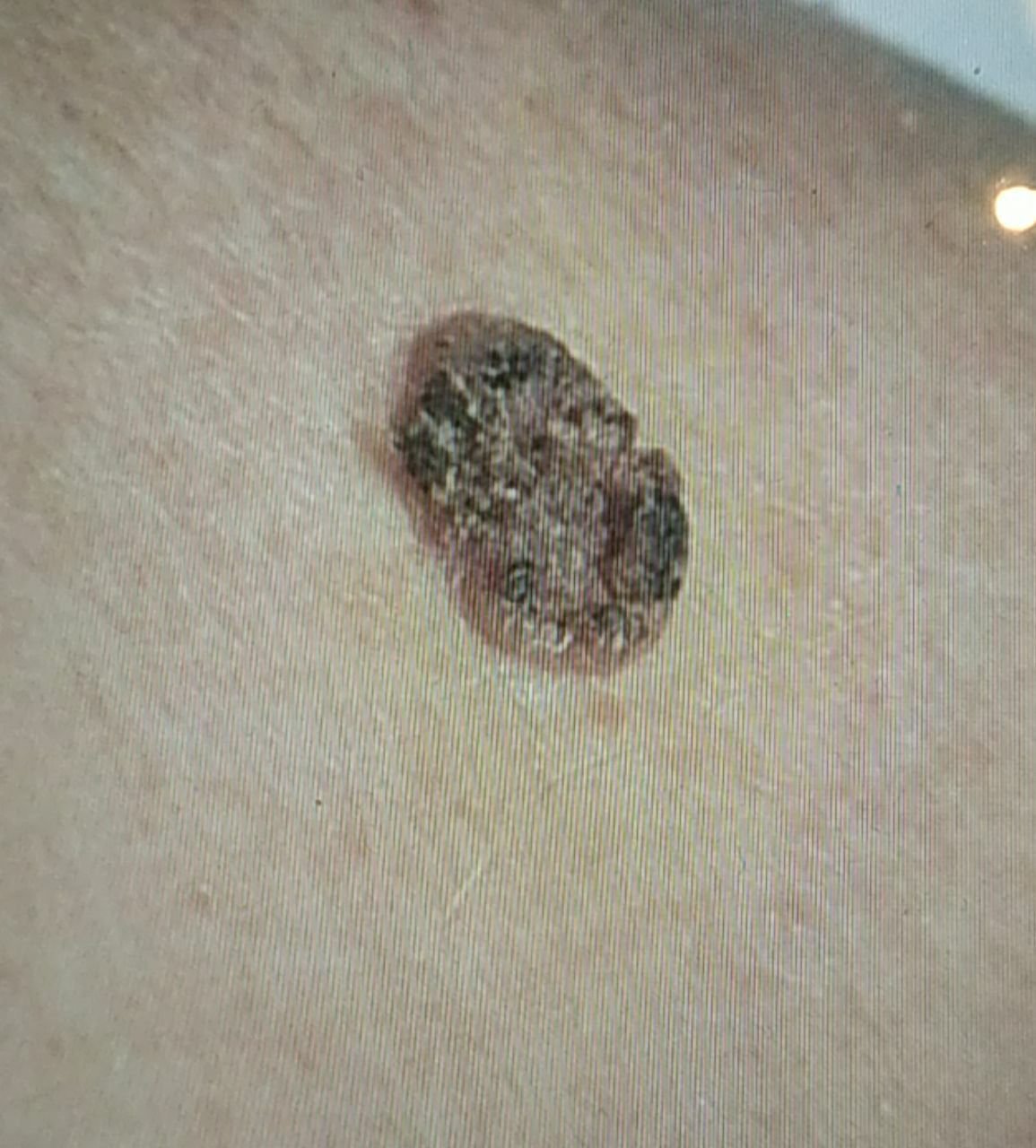
During a visual examination, seborrheic keratosis appears as a flattened, hemispherical, or short-stalked lesion that rises above the skin. These lesions are often symmetrical, typically oval or round, although larger ones can have irregular shapes. The surface texture of seborrheic keratosis differs from that of normal skin: it is rough, dry, and may show signs of peeling. In some cases, especially for larger lesions over 10 mm, the surface may have a warty texture, resembling large, uneven dry papillae. In certain instances, the keratinization is so pronounced that parts of the keratosis may fall off on their own or with minimal physical impact.
The boundaries of seborrheic keratosis are usually clear and even. However, in large keratomas, the edges can be uneven. The color of seborrheic keratosis varies from nude or gray to gray-brown. In some cases, shades of pink or pink-red may appear. Surrounding the lesion, the unchanged skin might show slight redness.
Hair growth in the area of seborrheic keratosis is typically not affected. However, in some cases, hair may grow in the lesion if it is congenital, or in the areas of keratomas with hypopigmentation.
The size of seborrheic keratosis varies, ranging from 5 mm to 20 mm in diameter. Lesions larger than 15 mm are rare. The height of the lesion above the skin surface usually does not exceed 5-7 mm.
On palpation, seborrheic keratosis feels dense and dry, with some areas potentially showing peeling. There are usually no subjective sensations, although mild itching may occur, especially in long-standing lesions.
Seborrheic keratosis is most commonly located on the trunk, upper limbs, and face. In older individuals, these lesions may also appear on other parts of the body.
Dermatoscopy of seborrheic keratosis reveals the following characteristic features:
It is important to differentiate seborrheic keratosis from other pigmented skin neoplasms, such as:
Seborrheic keratosis is generally a harmless condition, with a low risk of malignancy. Malignant transformation is rare but can occur, especially when the lesion is subjected to chronic injury or irritation, such as thermal burns or chemical exposure. The risk of malignant degeneration of seborrheic keratosis is estimated at 1-10%, with the majority transforming into squamous cell carcinoma. In some cases, this transformation may progress through a phase known as Bowen’s disease (a precancerous condition).
Patients with multiple seborrheic keratoses have an increased risk of developing other malignancies, particularly on the surrounding skin or in adjacent areas. This can complicate the timely detection and differential diagnosis of malignant lesions.
If no signs of damage, changes in appearance, or symptoms are present, self-monitoring is generally sufficient for seborrheic keratosis. This should include periodic checks, at least once a year. If mechanical damage occurs, or if any changes in the lesion are noticed, it is important to consult with a dermatologist or oncologist immediately.
The healthcare provider will assess whether further monitoring or removal of the lesion is necessary. Nevi that are constantly exposed to chronic trauma due to clothing, jewelry, or occupational activities should be considered for removal. Removal is also indicated if the patient experiences cosmetic discomfort or psychological distress.
For dynamic monitoring, it is helpful to take photos of the seborrheic keratosis to track any changes in appearance over time. Patients with multiple seborrheic keratoses should be evaluated by a dermatologist or oncologist in the spring and autumn (before and after the beach season). A skin neoplasm map is a valuable tool for ongoing observation, helping to identify new or altered lesions.
The treatment of seborrheic keratosis is typically surgical, including excision with either a classic scalpel or a radiofrequency scalpel. A histological examination of the excised tissue is necessary to confirm that the lesion is benign.
Less invasive methods, such as laser removal or cryodestruction (removal by liquid nitrogen), may be used after ensuring that the lesion is benign through a thorough examination by an oncologist or dermatologist. These methods should only be used after ruling out malignant transformation and performing a differential diagnosis.
If the lesion cannot be treated using less invasive methods, or if there are doubts about its nature, surgical excision remains the most effective option for removal. In some cases, patients may require multiple treatments due to the possibility of recurrence, particularly in congenital seborrheic keratosis.
Preventing the appearance of seborrheic keratosis and its potential for malignancy involves careful skin care and lifestyle adjustments:
Regularly inspecting seborrheic keratoses, seeking timely consultation with a healthcare specialist if any changes occur, and removing potentially dangerous lesions when necessary are essential for maintaining skin health.