Squamous cell carcinoma (SCC) is a type of malignant tumor that arises from the squamous cells located in the epidermis—the outermost layer of the skin. This cancerous formation is characterized by its aggressive behavior, including penetration into the deeper layers of the skin (dermis) and potential for extensive local tissue destruction. Although the tumor develops initially in the skin, it can progressively invade underlying structures, leading to disfigurement and complications. One of the major concerns associated with SCC is its potential to metastasize—that is, to spread to regional lymph nodes and distant organs, which significantly affects the patient’s prognosis and treatment strategy.
SCC typically begins to appear in individuals over the age of 35 to 40 years, although it may occur earlier in those with a history of chronic sun exposure or genetic predisposition. The condition affects men and women at approximately the same frequency and can arise on any part of the skin, although sun-exposed areas are more commonly affected. Early diagnosis and timely medical intervention are key to reducing the risks associated with this form of skin cancer.
While no single cause of squamous cell carcinoma has been definitively established, researchers and clinicians have identified several contributing factors that can significantly raise the risk of its development. These predisposing elements vary in severity and impact but often act cumulatively over time to damage the skin’s cellular integrity and encourage malignant transformation.
Accurate and early diagnosis of SCC is critical to improving treatment outcomes and minimizing the risk of metastasis. The diagnostic process typically begins with a thorough clinical examination of the affected area, during which a healthcare provider inspects the lesion’s size, shape, surface features, and rate of progression. The use of dermatoscopy enhances this process by providing a magnified view of sub-surface skin structures and vascular patterns.
If a lesion appears suspicious for SCC, the next essential step is a skin biopsy. This involves removing a portion or the entirety of the abnormal area for histopathological examination under a microscope. This allows a pathologist to confirm the diagnosis, determine the degree of cellular atypia, evaluate the depth of invasion, and assess whether additional tests are needed to detect metastasis.
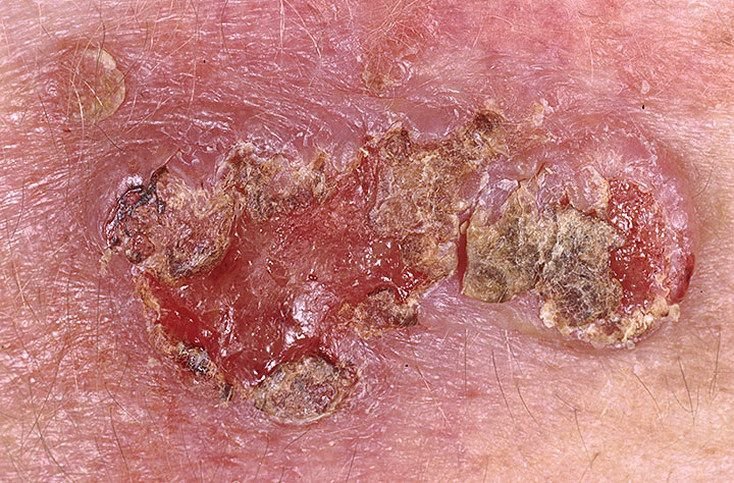
Squamous cell carcinoma can present in a number of forms, which can sometimes make it difficult to distinguish from other benign or less aggressive skin conditions. The tumor often appears as a persistent, thickened plaque or a nodule that protrudes from the surface of the skin. The lesion may have a rough, scaly, or wart-like texture and is commonly covered by crusts or horny (keratinized) masses. In more advanced cases, ulcers and areas of tissue breakdown (necrosis) may be visible, often with a characteristic yellow-gray coloration.
The borders of the tumor tend to be irregular and poorly defined, reflecting its infiltrative growth pattern. Although many SCCs are asymmetrical and misshapen, some may exhibit a regular round or oval contour. Lesions may appear as crateriform ulcers (with central depression) or dome-shaped growths anchored to the skin by a broad base.
The typical color is pink to reddish-pink, though gray tones may develop as keratin accumulates. Lesions often bleed easily with minor trauma, and surrounding skin may become hardened or inflamed. Notably, SCC lesions do not support hair growth due to follicular destruction.
The size of SCC lesions can range from as small as 4 mm to over 40 mm, depending on the duration of disease and absence of treatment. In cases of rapid growth, the tumor may spread across large anatomical regions. Palpation typically reveals a firm, indurated mass that is clearly distinct from the softer surrounding tissues.
Although early lesions are usually painless, discomfort and pain may develop if the tumor invades nerves or subcutaneous structures.
About 70% of SCCs are located on the face, scalp, and neck, making sun-exposed areas the most common sites. The rest appear on the trunk and extremities.
Dermatoscopy is an invaluable tool in the diagnosis of SCC. Several characteristic features can be visualized with this method, including:
Because of its varied appearance, SCC can be confused with several benign and malignant skin conditions. Accurate differentiation is essential to avoid mismanagement. Key conditions considered in differential diagnosis include:
Squamous cell carcinoma is a malignant tumor, and therefore carries all the serious implications associated with cancerous growths. Even when the tumor is surgically removed, there remains a substantial risk of local recurrence, particularly if the excision was incomplete or if the tumor had already invaded deeper tissue layers. The chances of metastasis—especially in neglected or advanced cases—add another level of clinical concern. The later SCC is diagnosed and treated, the more likely it is to spread beyond the skin, making early intervention crucial.
Metastases usually affect the regional lymph nodes that are nearest to the site of the primary tumor. However, in more advanced cases, cancer cells can travel through the bloodstream or lymphatic system to invade distant organs such as the lungs, liver, or bones.
Importantly, SCC can develop not only on previously healthy skin but also in areas where there are precancerous or benign lesions, such as actinic keratosis or chronic scars. In these instances, detecting malignant transformation can be more difficult and may delay appropriate treatment. This underlines the importance of careful, ongoing skin surveillance, especially in individuals with known risk factors.
Over the past decade, the incidence of SCC has shown a steady upward trend, increasing by approximately 10% every five years. Contributing factors include aging populations, greater exposure to UV radiation, and improved detection rates due to better screening techniques.
If there is any suspicion of squamous cell carcinoma—whether based on physical appearance, symptoms, or medical history—it is essential to promptly consult a dermatologist or oncologist. After an initial visual and dermatoscopic assessment, the physician may perform a biopsy to confirm the diagnosis through histological analysis.
In situations where the diagnosis is uncertain or the lesion is in a cosmetically sensitive area, doctors may opt for short-term active observation while documenting the lesion’s appearance. However, this is less common, and most suspected cases are biopsied without delay.
Once SCC is confirmed, the next step is a comprehensive staging evaluation to determine whether metastases are present. This might include ultrasound examination of lymph nodes, CT or MRI scans, and sometimes sentinel lymph node biopsy. Based on the findings, a personalized treatment protocol is established.
Because patients diagnosed with SCC are statistically at higher risk of developing additional skin cancers in the future, ongoing dermatological surveillance is recommended. This includes regular check-ups—at least twice per year—especially in spring and autumn when UV exposure varies most. The use of high-resolution photographs and digital mapping of skin lesions (mole mapping) is encouraged to help monitor changes over time and detect new suspicious formations early.
The cornerstone of treatment for squamous cell carcinoma is surgical excision of the tumor with clear margins. This approach involves removing the tumor along with a safety margin of healthy surrounding tissue to ensure complete elimination of cancer cells. Surgical removal remains the most effective method with a low rate of local recurrence when performed properly.
For tumors smaller than 20 mm or for patients who cannot undergo surgery, short-focus radiation therapy (superficial X-ray treatment) may be an appropriate alternative. This method is well-established and can be particularly useful for treating lesions in cosmetically or functionally sensitive areas, such as the nose, eyelids, or ears.
Other treatment methods—such as cryotherapy (freezing the tumor) or laser ablation—are not suitable for SCC, even at early stages. These superficial techniques do not allow for proper histological evaluation and often leave behind viable cancer cells, increasing the risk of recurrence or metastasis.
Some experimental protocols include the topical or localized application of cytostatic drugs (chemotherapy). While these treatments may provide good cosmetic results, they are not without controversy. Improper application may prolong the course of treatment, increase side effects, and fail to achieve complete tumor clearance. For this reason, such therapies must be administered strictly under medical supervision using clinically approved medications and protocols.
Preventing squamous cell carcinoma begins with a proactive and protective attitude toward your skin. While not all cases are avoidable, especially those linked to genetic or immunological factors, the vast majority can be prevented through common-sense skin care and lifestyle modifications. Key preventive measures include:
Early detection remains the most important factor in reducing SCC-related mortality. By combining protective behavior with professional dermatological oversight, the vast majority of SCC cases can be caught at a treatable stage and managed successfully.