Plane Wart (Flat Wart, Verruca Plana): Viral Skin Lesion with Benign Course
Overview
Plane warts, also known as flat warts or verruca plana, are benign epithelial tumors of viral origin caused by the human papillomavirus (HPV). These lesions are most frequently seen in children, adolescents, and young adults, and are characterized by their small size, flattened surface, multiplicity, and ability to resolve spontaneously in some cases—especially in younger individuals.
Despite being considered harmless, plane warts can cause significant cosmetic discomfort due to their location, which often includes exposed skin areas such as the face and hands. Moreover, warts can be resistant to treatment and may increase in number, leading to a need for medical intervention.
Predisposing Factors and Transmission
The causative agent of plane warts is HPV, usually of low oncogenic risk (e.g., types 3, 10, 28). However, while HPV infects a large portion of the population, not everyone develops visible lesions. This suggests that the manifestation of warts depends on individual susceptibility and immune status.
Factors that increase the risk of developing flat warts include:
- Immunosuppression: Including HIV infection, cancer treatment, or autoimmune disease;
- Endocrine and metabolic disorders: Diabetes mellitus, obesity, or chronic nutritional deficiencies;
- Pregnancy: Hormonal and immune changes may promote wart growth;
- Chronic infections and stress: Weaken the immune system and favor HPV activation;
- Skin trauma: Micro-injuries or scratching facilitate viral entry (autoinoculation);
- Poor hygiene and close contact: Shared hygiene tools, direct skin contact, or contaminated surfaces;
- Pediatric population: Due to high rates of close physical interaction and thinner skin.
Transmission occurs through direct contact with infected skin or contaminated objects, and the virus can spread to adjacent areas through autoinoculation.
Diagnosis of Flat Warts
The diagnosis of plane warts is mainly clinical, relying on visual inspection of the skin. These lesions have a characteristic appearance, allowing experienced dermatologists to make a diagnosis during a physical exam.
Additional tools may be used in complex or atypical cases:
- Dermatoscopy: Helps visualize subtle vascular and keratinization patterns typical of plane warts;
- HPV typing: May be conducted to identify specific strains, especially in recurrent or treatment-resistant cases;
- Skin biopsy: Performed when malignancy is suspected or the lesion does not respond to standard therapy. Histological examination reveals acanthosis, hyperkeratosis, and koilocytosis.
Symptoms and Clinical Features
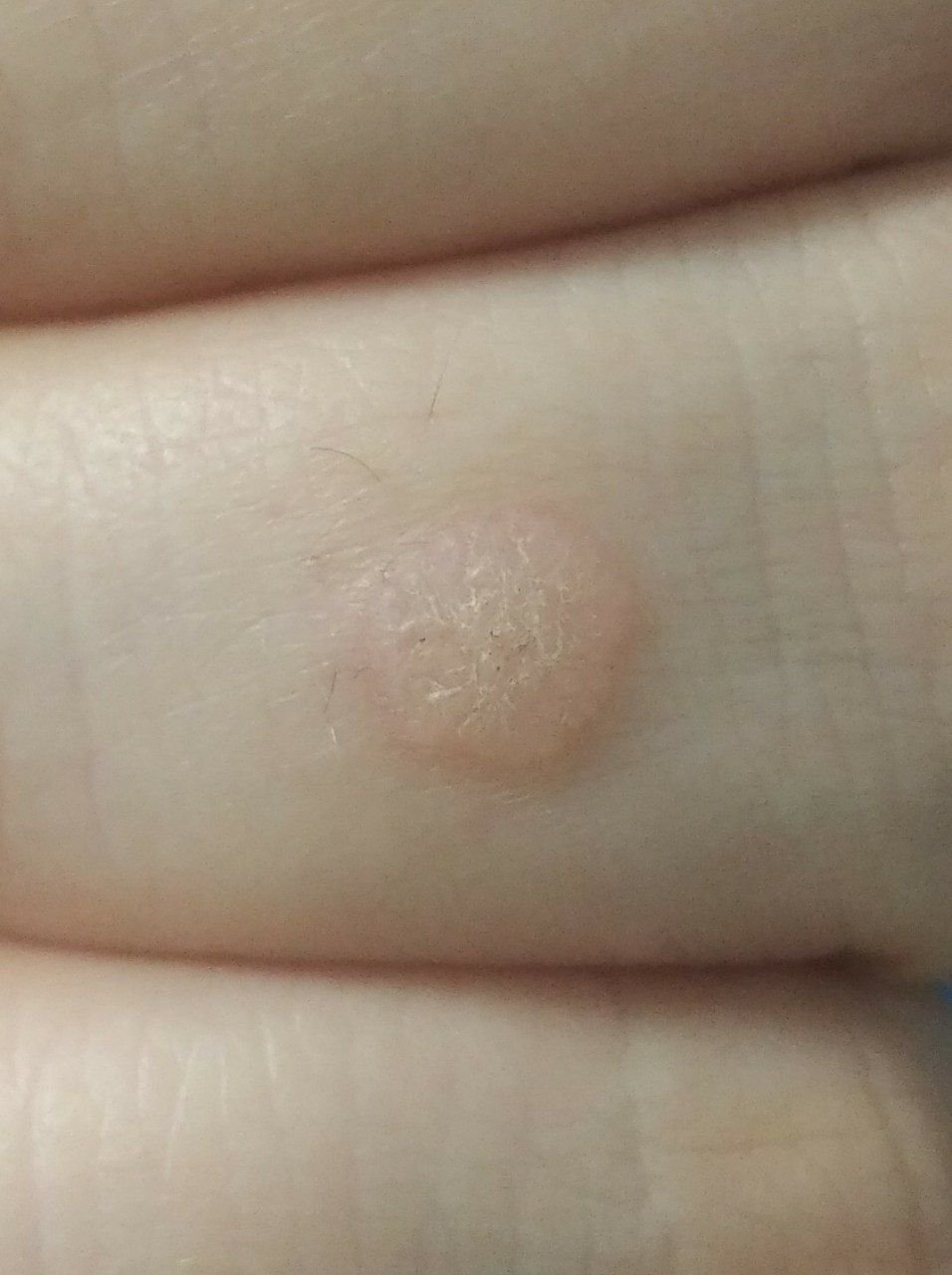
Flat warts present as small, slightly elevated lesions with a smooth, flattened surface. They often occur in clusters or linear patterns due to the Koebner phenomenon (appearance of new lesions after trauma). Their color ranges from skin-colored to pale brown or grayish, depending on the degree of keratinization and sun exposure.
Key clinical features include:
- Size: Typically 2–5 mm in diameter and 1–2 mm in height;
- Texture: Soft, smooth, and slightly velvety to the touch;
- Margins: Clearly defined, often with a subtle corolla of elevated skin around the edge;
- Hair growth: Usually absent on the lesion itself;
- Location: Commonly seen on the face, forehead, cheeks, chin, back of hands, forearms, and shins;
- Symptoms: Asymptomatic in most cases; rarely, mild tingling or irritation on pressure may occur.
Dermatoscopic Description
Dermatoscopy can aid in distinguishing flat warts from other papular dermatoses. In the case of plane warts, the following structures are often observed:
- Lightly pigmented surface: With fine granularity and minimal keratin buildup;
- Reduced “frogspawn” pattern: Compared to common warts, central red dots (capillaries) are less vivid or less numerous;
- Black or brown dots: Represent thrombosed capillaries, more subtle in plane warts;
- Sharp demarcation: A pale border or horn ring may be visible between the lesion and healthy skin.
These dermoscopic findings are especially useful in differentiating flat warts from early basal cell carcinoma, seborrheic keratosis, and pigmented lesions.
Differential Diagnosis
Flat warts must be differentiated from a variety of benign and malignant skin lesions that can mimic their appearance. Accurate diagnosis is particularly important for atypical or resistant cases. The differential diagnosis includes:
- Papillomatous nevus: More irregular and pigmented than flat warts, often congenital in origin;
- Nevus sebaceous: Typically yellowish, waxy plaques found on the scalp or face in childhood;
- Halo nevus: Pigmented nevus with surrounding depigmented area, usually without keratinization;
- Dermatofibroma: Firm, brownish nodules that dimple inward when pinched;
- Common warts (verruca vulgaris): More raised and keratinized, often with rough surface and black dots;
- Plantar wart: Found on soles of the feet, deeper and often painful;
- Molluscum contagiosum: Dome-shaped lesions with central umbilication, softer on palpation;
- Nodular basal cell carcinoma: Slow-growing pearly nodule, may ulcerate or bleed;
- Amelanotic melanoma: Rare and non-pigmented malignant lesion, requires biopsy if suspected.
Risks and Clinical Relevance
Flat warts are considered oncologically safe and carry a negligible risk of malignancy. Nonetheless, patients should be educated to monitor for signs of transformation, especially in lesions that change in:
- Size (rapid or disproportionate growth);
- Color (darkening, irregular pigmentation);
- Texture (ulceration or excessive keratinization);
- Symptoms (onset of pain, bleeding, or inflammation).
Additional risks include:
- Cosmetic impact: Particularly in facial or visible locations;
- Trauma-related complications: On areas exposed to friction or mechanical irritation (e.g., hands, wrists);
- Autoinoculation: New lesions may form on adjacent skin through scratching or shaving;
- HPV carriage: Indicates a compromised immune defense or increased viral load, especially in cases of widespread lesions.
Tactics: Clinical Management and Monitoring
If flat warts are asymptomatic and not cosmetically disturbing, dermatologists may recommend dynamic observation with periodic re-evaluation—especially in children and adolescents, where spontaneous resolution is common.
However, a dermatologic consultation is warranted in the following scenarios:
- Lesions are multiplying or merging into clusters;
- There are changes in appearance or texture;
- Warts are traumatized or inflamed;
- There is significant aesthetic or psychological concern;
- The patient is immunocompromised or has chronic skin disorders.
Regular monitoring through photographic documentation and skin mapping is useful, especially for patients with multiple lesions or high recurrence risk. Examinations are recommended at least twice a year—before and after summer sun exposure.
Treatment of Flat Warts
Treatment aims to eliminate visible lesions, prevent recurrence, and avoid complications. Minimally invasive methods are preferred, especially for facial or cosmetically sensitive areas.
Common treatment methods include:
- Laser therapy: Effective for small clusters or cosmetically important areas;
- Cryotherapy: Application of liquid nitrogen, often requires multiple sessions;
- Electrocoagulation or curettage: Destruction of wart tissue under local anesthesia;
- Radiofrequency removal: Precise, less traumatic technique ideal for multiple lesions;
- Topical agents: Salicylic acid, retinoids, imiquimod, or other antiviral/keratolytic formulations (used under medical supervision);
- Surgical excision: Reserved for atypical lesions or cases with diagnostic uncertainty, followed by histopathological examination.
Self-removal is discouraged due to the risk of bleeding, infection, scarring, and viral dissemination. All procedures should be performed in sterile conditions by qualified professionals.
Prevention of Plane Warts
Prevention of verruca plana relies on minimizing exposure to HPV, maintaining healthy skin, and supporting immune function.
- Good hygiene: Avoid sharing personal care items (e.g., razors, towels);
- Immune health: Ensure adequate sleep, balanced nutrition, stress control, and physical activity;
- Skin protection: Prevent minor skin injuries and treat existing skin conditions promptly;
- UV protection: Use SPF on exposed skin and avoid excessive sun exposure or tanning beds;
- Limit contact with warts: Do not scratch, shave over, or manipulate lesions;
- Regular skin checks: Especially in high-risk individuals, including those with immune compromise or frequent viral skin lesions;
- HPV vaccination: Though designed for high-risk oncogenic strains, may offer partial protection or reduce transmission in certain cases.
With early identification, proper management, and education, most flat warts can be treated successfully—preventing cosmetic issues and reducing the spread of HPV within the population.