Revolutionizing Vitiligo Treatment: From Topical Creams to Oral JAK Inhibitors
Introduction
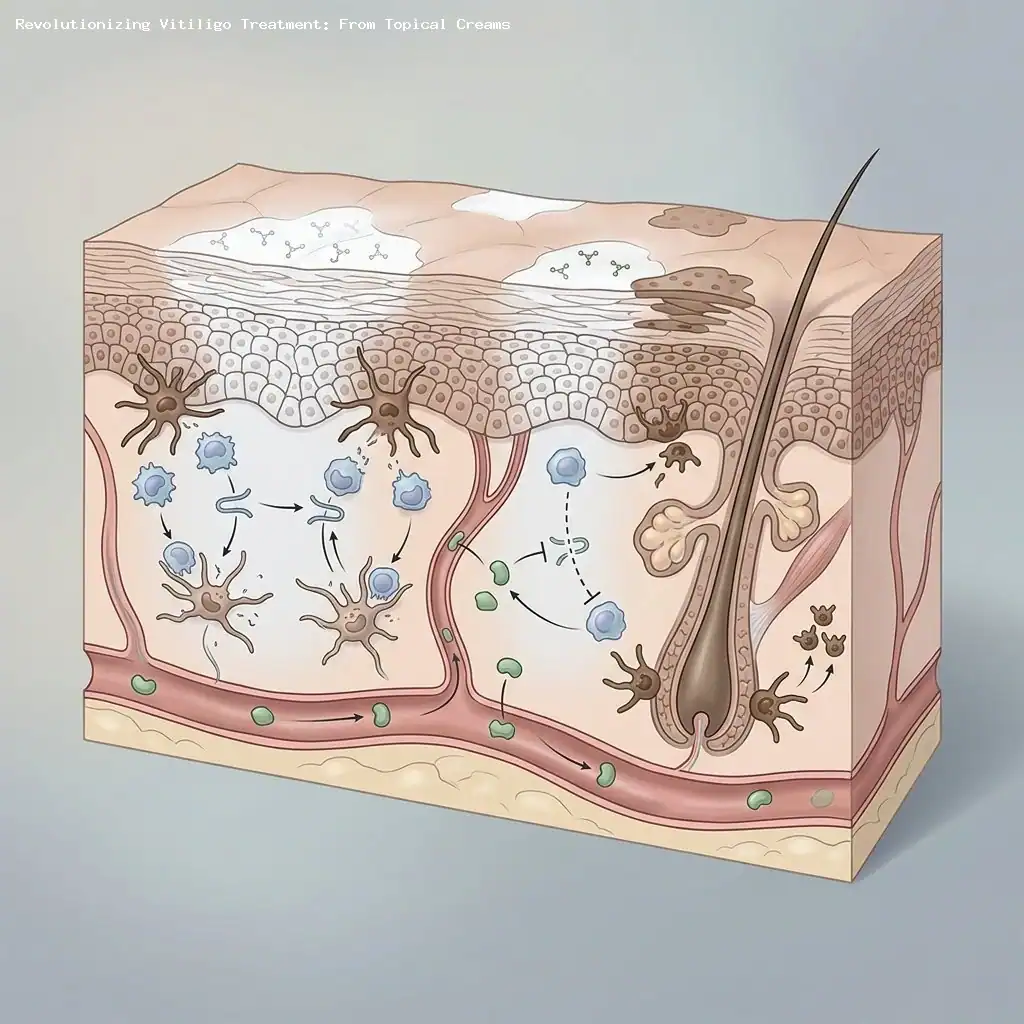
For many years, care for people with vitiligo relied largely on topical creams and phototherapy, with results that were often modest and unpredictable.
Recently, the arrival of targeted small molecules — especially oral Janus kinase (JAK) inhibitors — has begun to change that landscape by offering systemic options that address the immune processes that destroy pigment-producing melanocytes (Source: NEJM, TRuE-V Study Group).
These oral agents are particularly promising for people with extensive nonsegmental vitiligo (NSV), where treating large body-surface areas with creams is impractical and often less effective (Source: AbbVie press release, Phase 3 upadacitinib trials).
Limitations of Topical Therapies and Why Orals Matter
Topical medicines such as ruxolitinib cream have provided meaningful repigmentation for many patients, especially when vitiligo is limited to the face or small patches (Source: NEJM, TRuE-V Study Group).
In the pivotal TRuE‑V phase 3 trials, roughly 30% of patients using ruxolitinib cream reached at least a 75% improvement on the facial Vitiligo Area Scoring Index (F‑VASI75) at 24 weeks, compared with about 7%–11% on vehicle control — a statistically significant benefit (Source: NEJM, TRuE-V Study Group).
Longer follow-up showed increasing gains: at 52 weeks, just over half of patients who used ruxolitinib continuously from the start reached F‑VASI75, and about 30% achieved ≥90% facial repigmentation, with overall improvements in both face and total-body measures (Source: NEJM, TRuE-V Study Group).
Safety in the TRuE‑V program was generally acceptable; the most common side effects were application-site acne, itching, and upper respiratory symptoms, with serious treatment-related events being rare (Source: NEJM, TRuE-V Study Group).
Despite these advances, clinicians still report that achieving meaningful repigmentation across larger body-surface areas is challenging with topical-only approaches, which is a central reason why systemic oral therapies are being actively pursued (Source: NEJM, TRuE-V Study Group).
Upadacitinib: Leading the Oral JAK Revolution
Upadacitinib, an oral selective JAK1 inhibitor marketed as Rinvoq, is the first systemic oral to report positive phase 3 pivotal results in vitiligo, signaling a potential new standard for widespread disease (Source: AbbVie press release, Phase 3 upadacitinib trials).
In two replicate phase 3 studies of adolescents and adults with NSV, once‑daily upadacitinib 15 mg met both co‑primary endpoints at week 48: a ≥50% reduction in total VASI (T‑VASI50) and a ≥75% reduction in facial VASI (F‑VASI75), with treated patients showing markedly higher response rates than placebo (Source: AbbVie press release, Phase 3 upadacitinib trials).
Key secondary outcomes also favored upadacitinib; for example, nearly half of treated patients achieved a 50% facial VASI improvement at 48 weeks versus about 13% on placebo, demonstrating both facial and total-body benefits (Source: AbbVie press release, Phase 3 upadacitinib trials).
Safety observations were consistent with upadacitinib’s known profile from other inflammatory conditions: the most frequent treatment-emergent events included upper respiratory tract infections, acne, and nasopharyngitis, without new safety signals identified in the vitiligo studies (Source: AbbVie press release, Phase 3 upadacitinib trials).
Ritlecitinib: Broadening the Oral JAK Landscape
Ritlecitinib is an oral inhibitor targeting JAK3 and the TEC family kinases, and it has produced encouraging results in vitiligo trials that underscore both dose response and sustained benefit (Source: Yamaguchi et al., ritlecitinib study).
In a large, randomized phase 2b trial, ritlecitinib produced clear, dose-dependent repigmentation: the 50‑mg daily group showed significant percentage changes in F‑VASI at 24 weeks compared with placebo (for example, −21.2 vs 2.1; P < .001) (Source: Yamaguchi et al., ritlecitinib study).
Extension data out to 48 weeks showed continued repigmentation with ritlecitinib and did not reveal new or dose-limiting safety signals over that period, supporting its potential as a longer-term oral option for some patients (Source: Yamaguchi et al., ritlecitinib extension data).
Povorcitinib: Sustained Responses in Extensive Vitiligo
Povorcitinib, an oral selective JAK1 inhibitor, was tested in a phase 2b dose-ranging, placebo‑controlled trial in adults with extensive NSV and showed meaningful, sustained repigmentation (Source: Pandya et al., povorcitinib study).
At week 24, all povorcitinib dose groups (15 mg, 45 mg, and 75 mg once daily) demonstrated greater mean percent improvements in T‑VASI from baseline (about −15.7% to −19.1%) compared with only a 2.3% improvement for placebo, with each dose meeting statistical significance (P < .01) (Source: Pandya et al., povorcitinib study).
Importantly, repigmentation continued to deepen through one year: by week 52 the mean percentage change in T‑VASI approached −40% to −43% across doses, indicating durable and increasing benefit with ongoing therapy (Source: Pandya et al., povorcitinib study).
Emerging Systemic Orals and Combination Strategies
Beyond these JAK inhibitors, other systemic oral agents and different mechanisms are under study for vitiligo, expanding the therapeutic toolbox under investigation (Source: ClinicalTrials.gov, ViTYK trial information).
Deucravacitinib (a TYK2 inhibitor) and baricitinib (a JAK1/2 inhibitor) are examples of additional oral agents being explored in earlier-stage studies for vitiligo, though full phase 3 results are not yet public (Source: ClinicalTrials.gov, ViTYK trial information).
Researchers are also testing combinations of systemic agents with narrowband UV‑B (nbUV‑B) phototherapy to see whether immune modulation plus controlled light exposure can accelerate or deepen repigmentation; early presentations and pilot studies suggest potential added benefit that warrants larger trials (Source: Guttman‑Yassky, conference presentation).
Outside the JAK/TYK pathways, treatments that directly stimulate pigment production are being evaluated as complements to immunomodulation. For example, afamelanotide (an MC1R agonist) implanted to boost melanogenesis combined with nbUV‑B phototherapy has shown promise in prior randomized trials and remains under investigation as part of multimodal strategies (Source: Lim et al., JAMA Dermatology trial on afamelanotide plus nbUV‑B).
Clinical Implications and Practice Considerations
These oral systemic therapies signal a practical shift for clinicians treating people with extensive or treatment-refractory vitiligo: they offer the possibility of deeper and more widespread repigmentation than topical agents alone (Source: AbbVie press release; NEJM, TRuE‑V Study Group).
When interpreting trial results, it helps to understand common endpoints used in vitiligo studies: T‑VASI50 denotes a 50% reduction in total-body Vitiligo Area Scoring Index, while F‑VASI75 indicates a 75% improvement on the face — both are clinically meaningful measures of repigmentation that regulators and clinicians use to compare treatments (Source: NEJM, TRuE‑V Study Group; AbbVie press release).
Choosing a patient for systemic therapy involves weighing disease extent, rate of progression, prior treatment response, comorbidities, and individual risk tolerance: systemic JAK inhibitors modulate immune pathways and can carry infection and other safety considerations that need discussion and monitoring (Source: AbbVie press release; Yamaguchi et al.; Pandya et al.).
As manufacturers and regulators work through pivotal data and approval processes, clinicians will also need to consider practical issues such as long‑term safety data, insurance coverage, and patient preferences around pill-based versus topical or phototherapy regimens; many approvals and coverage decisions are anticipated in the 2026–2027 timeframe (Source: AbbVie press release; Pandya et al.).
Conclusion
The therapeutic landscape for vitiligo is evolving quickly: potent topical JAK inhibitors have helped many patients, but systemic oral agents — led by selective JAK1 and JAK3/TEC inhibitors — are now showing the potential for wider, deeper, and more durable repigmentation in people with extensive disease.
Ongoing research into other oral pathways, combination approaches with nbUV‑B, and agents that directly stimulate pigment production promises additional options in the coming years, but thoughtful patient selection and attention to safety will remain essential as these treatments enter practice (Source: NEJM, TRuE‑V Study Group; AbbVie press release; Pandya et al.).
Sources
- Rosmarin D, Passeron T, Pandya AG, et al; TRuE‑V Study Group. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. New England Journal of Medicine. 2022;387(16):1445-1455. (Source: NEJM, TRuE‑V Study Group)
- AbbVie. AbbVie announces positive topline results from phase 3 pivotal studies evaluating upadacitinib (RINVOQ) in adults and adolescents with vitiligo. Press release, October 29, 2025. (Source: AbbVie press release, Phase 3 upadacitinib trials)
- Yamaguchi Y, Peeva E, Duca ED, et al. Ritlecitinib, a JAK3/TEC family kinase inhibitor, stabilizes active lesions and repigments stable lesions in vitiligo. Phase 2b randomized trial. (Source: Yamaguchi et al., ritlecitinib study)
- Pandya AG, Ezzedine K, Passeron T, et al. Efficacy and safety of the oral Janus kinase 1 inhibitor povorcitinib in patients with extensive vitiligo: a phase 2, randomized, double‑blinded, dose‑ranging, placebo‑controlled study. (Source: Pandya et al., povorcitinib study)
- Vitiligo treatment by targeting TYK2 mediated responses (ViTYK). ClinicalTrials.gov identifier NCT06327321. Updated March 27, 2025. (Source: ClinicalTrials.gov, ViTYK trial information)
- Guttman‑Yassky E. Oral ritlecitinib plus nbUV‑B accelerates repigmentation in nonsegmental vitiligo. Conference presentation. (Source: Guttman‑Yassky, conference presentation)
- Lim HW, Grimes PE, Agbai O, et al. Afamelanotide and narrowband UV‑B phototherapy for the treatment of vitiligo: a randomized multicenter trial. JAMA Dermatology. (Source: Lim et al., JAMA Dermatology trial)