Rosacea Explained: New Insights and Emerging Treatments in 2024
Rosacea Awareness Month: Why April Matters
Each April, Rosacea Awareness Month invites patients, clinicians, and the public to take a fresh look at a skin condition that’s common but often misunderstood.
Even though rosacea is a frequent diagnosis in dermatology clinics, research over the last several years shows that our picture of the disease is still changing, with new insights into what causes it and how to treat it (Source: Fisher GW et al., Frontiers in Medicine, 2023).
Pathophysiology: What’s Happening Under the Skin
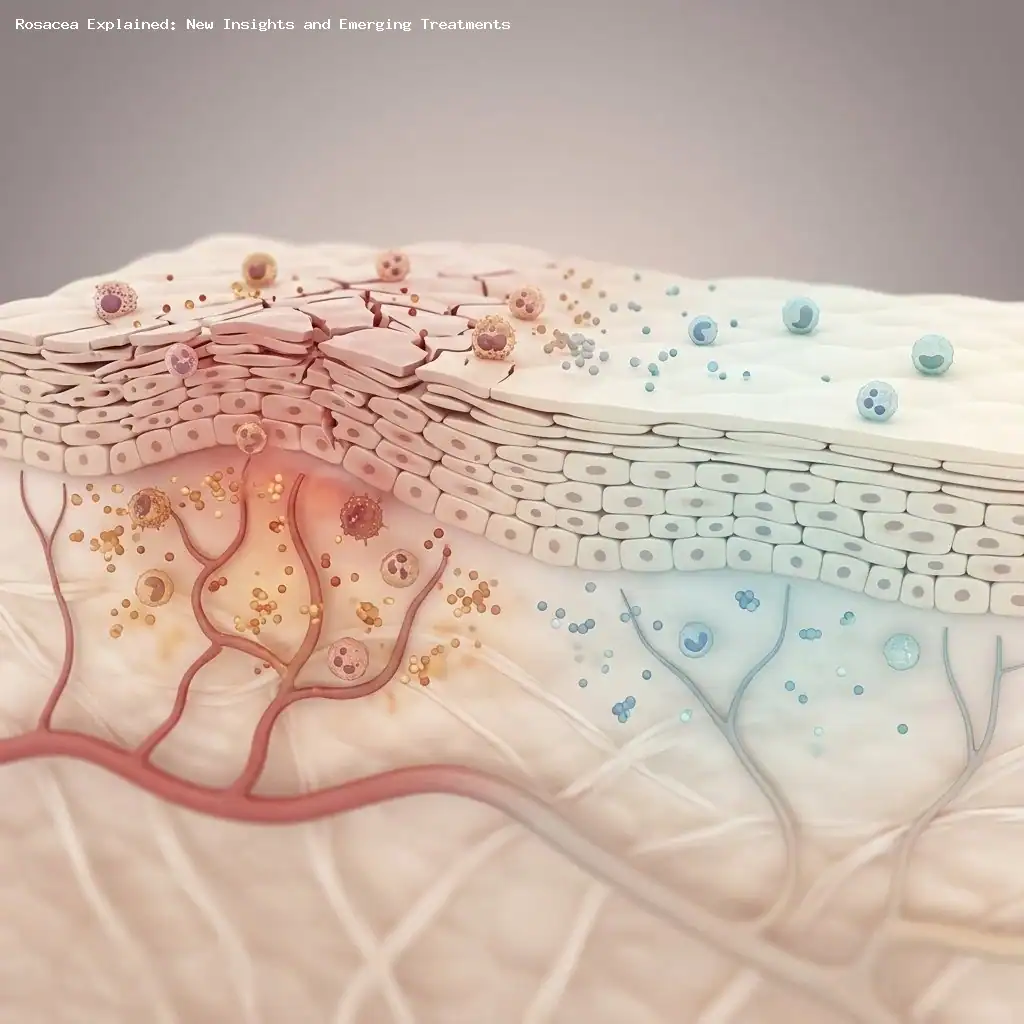
Rosacea is best understood as a chronic inflammatory skin disorder driven by multiple overlapping factors rather than a single cause (Source: Advances in the pathogenesis of rosacea, Frontiers in Immunology, 2025).
Key contributors to rosacea include a mix of genetic predisposition, immune dysregulation, neurovascular dysfunction, skin barrier impairment, and environmental influences (Source: Yang F et al., Frontiers in Immunology, 2024).
Growing evidence points to interactions between innate immune activation, proinflammatory cytokine release, and abnormal new blood vessel formation (angiogenesis) as central drivers of persistent facial redness and exaggerated flushing (Source: Fisher GW et al., Frontiers in Medicine, 2023).
Clinical Subtypes
Clinically, rosacea is often grouped into four subtypes to help guide treatment, though many people have features of more than one type (Source: Mohamed-Noriega K et al., Ocular Rosacea review).
-
Papulopustular rosacea: centered on inflammatory papules and pustules across the central face.
-
Erythematotelangiectatic rosacea: persistent midface redness with visible small blood vessels (telangiectasias) and recurrent flushing.
-
Phymatous rosacea: tissue thickening and enlargement, often with sebaceous gland overgrowth; more commonly seen in men.
-
Ocular rosacea: affects the eyelids and surface of the eye with symptoms like burning, stinging, dryness, and a gritty sensation; exam may show lid margin telangiectasias and conjunctivitis (Source: Mohamed-Noriega K et al., Ocular Rosacea review).
Because overlap is common, treatment should be tailored to the individual’s combination of symptoms rather than rigidly to a single subtype (Source: Nguyen C et al., Clinical guidance).
Common Exacerbating Factors
Rosacea is famously sensitive to environmental and lifestyle triggers, and identifying personal triggers is a cornerstone of long-term control (Source: National Rosacea Society).
-
Ultraviolet (UV) exposure and sunlight.
-
Temperature extremes: heat, cold, and wind.
-
Emotional stress and intense physical exertion.
-
Alcohol (especially red wine), very hot drinks, and spicy foods.
-
Skin care products that contain alcohol or fragrance, or misuse of topical corticosteroids.
-
Certain medications that dilate blood vessels and hormonal changes such as menopause.
Tracking flares and modifying exposures remains one of the most practical and effective ways to reduce symptoms over time (Source: National Rosacea Society).
Management Principles: Start with the Skin Barrier
Foundational care focuses on restoring and protecting the skin barrier, since barrier breakdown fuels inflammation and sensitivity (Source: Skin barrier in rosacea, Anais Brasileiros de Dermatologia).
Simple, practical steps include using a gentle cleanser that maintains the skin’s natural pH, applying a daily moisturizer to reduce water loss, and using a mineral-based sunscreen (SPF ≥ 30) to limit UV-triggered inflammation (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
These low-risk measures often improve tolerance to medical treatments and help reduce flare frequency and severity (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
Current Therapeutic Options
Topical Therapies
A variety of FDA-approved topical agents address different rosacea features; choice depends on whether redness, bumps, or both are dominant (Source: product labeling; Galderma; Allergan).
-
Brimonidine (Mirvaso; Galderma) — primarily for temporary vasoconstriction and reduction of persistent erythema.
-
Oxymetazoline (Rhofade; AbbVie/Allergan) — another topical vasoconstrictor for facial redness.
-
Ivermectin (Soolantra; Galderma) — anti-inflammatory with activity that may reduce Demodex mite–associated inflammation.
-
Azelaic acid (Finacea; Bayer) — reduces inflammation and lesion count.
-
Sodium sulfacetamide/sulfur (Avar; Mission Pharmacal) — useful for inflammatory lesions and for Demodex-targeted therapy.
-
Metronidazole (MetroGel; Galderma) — a longstanding anti-inflammatory topical option.
-
Encapsulated benzoyl peroxide (Epsolay; Sol-Gel Technologies) — designed to reduce irritation while targeting inflammatory lesions.
-
Topical minocycline (Zilxi; Foamix Pharmaceuticals) — a newer topical antibiotic formulation for papulopustular disease.
Topical vasoconstrictors like brimonidine and oxymetazoline are particularly useful for persistent redness, while anti-inflammatory and antiparasitic topicals target papules, pustules, and Demodex-associated inflammation (Source: product labeling; Fisher GW et al., Frontiers in Medicine, 2023).
Oral Therapies
Systemic options are typically used for moderate-to-severe inflammatory rosacea or when topical regimens are insufficient (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
-
Tetracyclines — doxycycline and minocycline remain mainstays because of their anti-inflammatory effects rather than pure antibiotic action.
-
Modified-release doxycycline (Oracea; Galderma) and modified-release minocycline (Emrosi; Journey Medical) provide anti-inflammatory benefits at lower doses.
-
Low-dose isotretinoin (Accutane; Roche) — an option for refractory papulopustular or phymatous disease but requires strict monitoring because of teratogenicity.
-
Off-label use of β-blockers (for example, propranolol or carvedilol) may help reduce flushing and persistent erythema in selected patients (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
Choice among oral agents depends on disease severity, reproductive plans, comorbidities, and prior response to treatments, so discussion with a clinician is essential (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
Procedural Interventions
For visible blood vessels, stubborn redness, or tissue thickening, laser and light-based therapies are important tools (Source: Husein-ElAhmed H & Steinhoff M, systematic review).
-
Pulsed dye laser — effective for telangiectasias and persistent erythema.
-
Nd:YAG laser — useful for deeper vessels and thicker telangiectasias.
-
For phymatous rosacea, options include CO2 ablative laser and electrosurgery to debulk excess tissue and reshape contours.
Clinical trials and meta-analyses support laser approaches for reducing vessel visibility and erythema, though multiple sessions and maintenance may be needed (Source: Husein-ElAhmed H & Steinhoff M; Frontiers in Medicine meta-analysis, 2021).
Emerging Therapies: What’s on the Horizon
Despite many available treatments, unmet needs remain—especially for persistent erythema and cases that don’t respond to standard therapy (Source: Fisher GW et al., Frontiers in Medicine, 2023).
IL-17 Inhibitors and Biologics
Heightened levels of proinflammatory cytokines and angiogenic signals have been documented in rosacea-affected skin, suggesting a role for targeted biologic therapy (Source: Yang F et al., 2024).
Agents that block IL-17, such as secukinumab (Cosentyx; Novartis), are being explored for their ability to specifically modulate inflammatory pathways implicated in rosacea and may offer a precision approach for select patients (Source: clinical research literature; Novartis pipeline reports).
JAK Inhibitors
The JAK-STAT pathway—notably JAK2/STAT3 signaling—has been implicated in rosacea-related cytokine production, and early trials of JAK inhibitors show promise for reducing facial redness (Source: Yang F et al., 2024).
For example, investigational use of oral tofacitinib (Xeljanz; Pfizer) produced substantial reductions in facial erythema in early reports, suggesting a potential new avenue for therapy pending larger, controlled studies (Source: Yang F et al., Signaling pathways and targeted therapy for rosacea, 2024).
These targeted approaches are still experimental for rosacea but represent a shift toward treating underlying immune pathways rather than only symptoms (Source: Fisher GW et al., Frontiers in Medicine, 2023).
Putting It All Together: A Practical Approach
Successful rosacea care combines trigger management, barrier repair, appropriate topical and/or oral medications, and procedural therapies when needed (Source: Oge’ LK et al., Rosacea: diagnosis and treatment).
Treatment decisions should be individualized—taking into account the dominant symptoms, disease severity, tolerance of therapies, and patient goals—because rosacea often presents differently from person to person (Source: Nguyen C et al., Practical guidance and challenges for clinical management).
As our understanding of the immune and vascular contributors to rosacea grows, newer targeted treatments may offer more durable control for patients who do not respond adequately to current options (Source: Fisher GW et al., Frontiers in Medicine, 2023).
About the Author
Jill Cowan, APRN, FNP-BC, is a board-certified nurse practitioner practicing dermatology in Cincinnati.
She focuses on patient-centered, evidence-based care and contributes to clinical education and writing on skin disease management.
Sources
- Fisher GW, Travers JB, Rohan CA. “Rosacea pathogenesis and therapeutics: current treatments and a look at future targets.” Frontiers in Medicine (Lausanne), 2023. (Source: Frontiers in Medicine)
- “Advances in the pathogenesis of rosacea.” Frontiers in Immunology, 2025. (Source: Frontiers in Immunology)
- Yang F, Wang L, Song D, et al. “Signaling pathways and targeted therapy for rosacea.” Frontiers in Immunology, 2024. (Source: Frontiers in Immunology)
- Mohamed-Noriega K, Loya-Garcia D, Vera-Duarte GR, et al. “Ocular rosacea: an updated review.” (Source: Ophthalmology literature)
- Frazier W, Zemtsov RK, Ge Y. “Rosacea: common questions and answers.” (Source: Clinical review literature)
- Nguyen C, Kuceki G, Birdsall M, Sahni DR, Sahni VN, Hull CM. “Rosacea: practical guidance and challenges for clinical management.” Clinical, Cosmetic and Investigational Dermatology. (Source: Clin Cosmet Investig Dermatol)
- National Rosacea Society. “Factors that may trigger rosacea flare-ups.” (Source: National Rosacea Society website)
- “Skin barrier in rosacea.” Anais Brasileiros de Dermatologia. (Source: Brazilian dermatology journal)
- Oge’ LK, Muncie HL, Phillips-Savoy AR. “Rosacea: diagnosis and treatment.” (Source: Clinical review literature)
- Husein-ElAhmed H, Steinhoff M. “Light-based therapies in the management of rosacea: a systematic review with meta-analysis.” International Journal of Dermatology. (Source: IJD systematic review)
- “Efficacy comparison of pulsed dye laser vs. microsecond 1064-nm Nd:YAG laser in the treatment of rosacea: a meta-analysis.” Frontiers in Medicine (Lausanne), 2021. (Source: Frontiers in Medicine)
- Product labeling and company information: Galderma (Mirvaso, Soolantra, MetroGel), AbbVie/Allergan (Rhofade), Bayer (Finacea), Mission Pharmacal (Avar), Sol-Gel Technologies (Epsolay), Foamix Pharmaceuticals (Zilxi), Roche (Accutane), Galderma (Oracea), Journey Medical (Emrosi), Novartis (Cosentyx), Pfizer (Xeljanz). (Source: Company product information and regulatory labels)