Tattoo Safety Today: What You Need to Know About Modern Ink Risks
Why dermatologists love—and worry about—tattoos
I’ve spent years enjoying the creativity that comes through my clinic doors: lifelike portraits, pop-culture icons, tiny floral sprigs and bold sleeves that tell a person’s story.
At the same time, the conversation around tattoos in dermatology has expanded well past simple questions about fading, allergic reactions, or localized infections from bacteria like Staphylococcus aureus.
For a long time many of us treated tattoos as a largely inert, permanent pigment lodged in the skin. But as tattooing has become more common, research and surveillance have caught up—and what we’re learning is making clinicians rethink how tattoos interact with the body.
Part of this shift was covered recently in a National Geographic deep dive into tattoo safety, which highlights concerns that move beyond skin-level issues into the realm of systemic disease and cancer risk (Source: National Geographic, “What to know about the link between tattoo ink and cancer risk”).
Epidemiology: new studies that change the conversation
Historically, tattoos were mainly discussed in dermatology as a cosmetic or local skin-care issue, but new population studies are reframing that view by examining long-term and systemic outcomes.
Most notably, a Swedish population-based case-control study reported a roughly 21% increased risk of lymphoma among people with tattoos compared with those without tattoos, a finding that has sparked careful attention in the dermatology and oncology communities (Source: Nielsen C et al., “Tattoos as a risk factor for malignant lymphoma: a population-based case-control study”).
That Swedish study also found a surprising time pattern: a U-shaped risk curve with a peak in lymphoid cancer risk in the first two years after tattooing and another rise after 11 or more years—suggesting both an early immune response and a possible late, chronic effect (Source: Nielsen C et al.).
Other studies looking at melanoma and nonmelanoma skin cancer have produced mixed results: some North American and European analyses have not shown clear increases in melanoma risk, and a few even reported paradoxical findings like lower melanoma risk after multiple tattoo sessions (Source: Rietz Liljedahl E et al.; Mo T et al.; McCarty RD et al.; Karregat JJJP et al.).
But the pattern is not limited to one country. A Danish twin cohort reinforced concerns about lymphoma and skin cancers linked to tattoo exposure, especially when tattoos are large—bigger than a human palm in some analyses—adding weight to the idea that exposure size may matter (Source: Clemmensen SB et al.).
The lymphatic story: pigment doesn’t just stay put
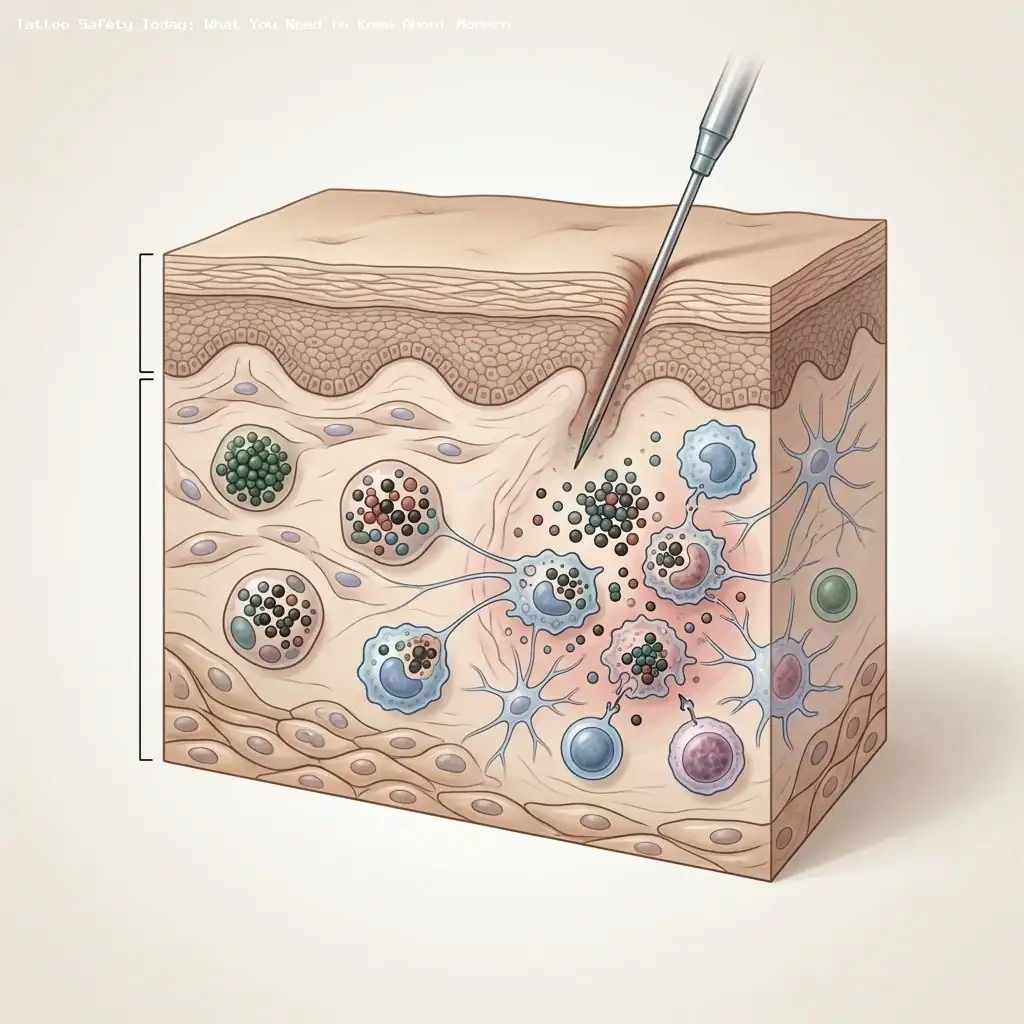
One of the most important shifts in our understanding is that tattoo pigment is not permanently trapped inside the dermis; it moves. Studies using animal models and tissue analysis show that pigment particles are taken up by immune cells and transported to regional lymph nodes (Source: Cambiaso-Daniel J et al.; Laux P et al.).
When macrophages carry ink to lymph nodes, the pigment particles can accumulate there—sometimes visibly changing node color—and create a persistent immune stimulus rather than a passive deposit (Source: Kluger N & Koljonen V; Laux P et al.).
Some tattoo inks contain heavy metals such as cadmium and lead, and particulate components such as polycyclic aromatic hydrocarbons (PAHs) and primary aromatic amines (PAAs), all of which can be biologically active and potentially harmful when concentrated in lymphoid tissue (Source: Negi S et al.; Violi JP et al.; Lehner K et al.).
There is concern that chronic immune activation within lymph nodes or localized chemical toxicity could contribute to genomic damage over time—one plausible pathway by which tattoo exposure might influence lymphoma risk—though the precise biology is still being studied (Source: Neale PA et al.; Capucetti A et al.).
Clinically, migrated pigment can also create confusion: pigmented lymph nodes may mimic metastatic disease on imaging or appear during sentinel node biopsy, which can complicate cancer staging and surgical planning (Source: Cambiaso-Daniel J et al.; Laux P et al.).
How tattoos change the full-body skin exam
A routine full-body skin exam (FBSE) is the backbone of skin cancer detection, but extensive tattooing makes that exam harder and forces clinicians to change how they look and what they rely on during evaluation.
Tattoo ink can mask or alter pigmented lesions, obscuring the classic visual cues we use to spot melanoma—our familiar ABCDE rules can be harder to apply when pigmentation is mixed in with ink.
For that reason, clinicians are advised to adapt their approach and emphasize alternative clues that are less affected by exogenous pigment: vascular features and structure rather than color alone (Source: Reis JM et al.).
Dermoscopic adjustments
Traditional dermoscopic markers of pigmented tumors—like network patterns and specific pigmented structures—may be hidden by tattoo dye. Recent reports recommend shifting focus to vascular morphology and shiny white structures, which can still be visible through ink and provide red flags for both melanoma and nonmelanoma skin cancers (Source: Reis JM et al.).
The “blackout” tattoo problem
Blackout tattoos—large swaths of solid black ink—pose a particular challenge because they eliminate visual contrast. In these cases, palpation (feeling for induration, nodularity, or textural change) and careful attention to patient-reported symptoms such as persistent pruritus or stinging are especially important.
When visual inspection is limited, a clinician’s threshold for using advanced diagnostic tools should be lower to avoid missed or delayed diagnoses.
When to use advanced imaging
Noninvasive imaging tools such as reflectance confocal microscopy (RCM) and optical coherence tomography (OCT) can be useful when tattoo ink hides surface clues; these technologies sometimes provide cellular- or subsurface-level information that helps decide whether a biopsy is needed (Source: clinical practice guidance and expert commentary).
Tattoo color, chemistry, and sunlight
Tattoo inks are chemically diverse, and color matters: black inks typically contain carbon black and may be contaminated with or include carcinogenic PAHs such as benzo(a)pyrene, while red inks often rely on azo dyes that can break down into primary aromatic amines (PAAs) (Source: Lehner K et al.; Negi S et al.).
Ultraviolet (UV) radiation introduces another layer of concern. UV exposure can induce photodecomposition of tattoo pigments, creating toxic byproducts and reactive oxygen species that could increase local and regional chemical stress (Source: Regensburger J et al.).
That means sun protection for tattooed skin isn’t only about preventing burns or fading color—it’s also about limiting chemical breakdown of ink and the formation of potentially harmful degradation products.
Laser removal: benefits and a possible trade-off
Laser tattoo removal is an increasingly common choice—but it’s not without biological effects. Breaking ink into smaller fragments can accelerate transport of particles to lymph nodes, possibly increasing lymphatic exposure to ink-derived chemicals (Source: Laux P et al.; Cambiaso-Daniel J et al.).
One analysis within the Swedish study cohort suggested higher rates of lymphoma among people who had undergone laser tattoo removal compared with those who had not, highlighting a complex risk–benefit balance that needs further exploration (Source: Nielsen C et al.).
Patients considering removal should discuss these potential trade-offs with a clinician, and removal should be performed by or in consultation with experienced providers who can explain the pros and cons.
Translating evidence into clinical practice
Tattoo ink is no longer just a cosmetic concern; it intersects with immunity, lymphatic biology, imaging, and cancer epidemiology. That reality calls for practical changes in how we counsel and care for patients.
Key practice steps clinicians can take include:
-
Pre-tattoo counseling: Encourage baseline skin exams before a person gets a large or new tattoo, and advise tattoo artists and clients to avoid inking directly over suspicious moles or surgical scars (Source: clinical consensus and expert recommendation).
-
Lymph node checks: Add focused lymph node palpation to the FBSE in heavily tattooed patients to look for new or persistent lymphadenopathy that could reflect pigment migration or pathology (Source: Laux P et al.; Cambiaso-Daniel J et al.).
-
Patient education on sun care: Reframe photoprotection messages to explain that sunscreen and sun avoidance also protect the chemical stability of tattoo pigments and may reduce formation of harmful breakdown products (Source: Regensburger J et al.).
-
Lower thresholds for imaging/biopsy: In cases where ink obscures examination, use RCM, OCT, or proceed to biopsy when clinical suspicion is present rather than waiting for classic visual signs (Source: Reis JM et al.; clinical practice guidance).
-
Discuss removal risks: When patients ask about laser removal, explain the potential for increased lymphatic transport of fragmented pigment and discuss alternatives and monitoring plans (Source: Laux P et al.; Nielsen C et al.).
Where the research needs to go next
Current findings raise important questions but do not yet provide definitive cause-and-effect answers. We need:
-
Long-term prospective studies that follow tattooed people over decades with clear measures of ink composition and removal history (Source: calls for further research across epidemiologic literature).
-
Laboratory work clarifying which ink components are biologically active, how they degrade in the skin, and what they do in lymph nodes at cellular and genomic levels (Source: Negi S et al.; Neale PA et al.).
-
Better regulatory oversight and standardized ingredient labeling for tattoo inks so clinicians and consumers can make informed choices (Source: policy and toxicology reviews).
Practical takeaway for patients
Tattoos are meaningful and widely accepted, and most people with tattoos will never develop cancer because of their ink. However, the emerging science suggests they are not biologically inert and that careful, informed decisions make sense.
If you have tattoos or are considering one, consider getting a baseline skin check, protecting your ink from the sun, talking to your artist about avoiding moles, and discussing the pros and cons of removal with a clinician if you’re considering that option (Source: clinical guidance and epidemiologic studies).
Final thoughts
Tattoo ink sits at the crossroads of art, personal expression, and biology. As clinicians and researchers learn more, the message is not to alarm but to inform—so that people can enjoy body art with realistic knowledge of its interactions with the immune system and how we screen for and manage potential risks.
Sources
- National Geographic. “What to know about the link between tattoo ink and cancer risk.” Accessed March 12, 2026. (Source: National Geographic)
- Nielsen C, Jerkeman M, Jöud AS. “Tattoos as a risk factor for malignant lymphoma: a population-based case-control study.” eClinicalMedicine. doi:10.1016/j.eclinm.2024.102649 (Source: Nielsen C et al.)
- Rietz Liljedahl E, Nielsen K, Engfeldt M, Saxne Jöud A, Nielsen C. “Does tattoo exposure increase the risk of cutaneous melanoma? A population-based case-control study.” 2025;40(12):1441-1453. doi:10.1007/s10654-025-01326-6 (Source: Rietz Liljedahl E et al.)
- Mo T, Zins M, Goldberg M, et al. “Tattoos and risk of cutaneous melanoma and nonmelanoma skin cancer in France.” doi:10.1093/jnci/djaf332 (Source: Mo T et al.)
- McCarty RD, Trabert B, Collin LJ, et al. “Tattooing and risk of melanoma: a population-based case-control study in Utah.” 2025;117(12):2495-2504. doi:10.1093/jnci/djaf235 (Source: McCarty RD et al.)
- Karregat JJJP, Schipper K, Wolkerstorfer A, et al. “Incidence of tattoo-associated melanoma in the Netherlands (1991-2023): a nationwide registry study.” doi:10.1159/000549503 (Source: Karregat JJJP et al.)
- Clemmensen SB, Mengel-From J, Kaprio J, Frederiksen H, von Bornemann Hjelmborg J. “Tattoo ink exposure is associated with lymphoma and skin cancers – a Danish study of twins.” doi:10.1186/s12889-025-21413-3 (Source: Clemmensen SB et al.)
- Kluger N, Koljonen V. “Tattoos, inks, and cancer.” Lancet Oncology commentary. doi:10.1016/S1470-2045(11)70340-0 (Source: Kluger N & Koljonen V)
- Laux P, Tralau T, Tentschert J, et al. “A medical-toxicological view of tattooing.” Lancet. 2016;387(10016):395-402. doi:10.1016/S0140-6736(15)60215-X (Source: Laux P et al.)
- Cambiaso-Daniel J, Luze H, Meschnark S, et al. “Tattoo pigment biokinetics in vivo in a 28-day porcine model: elements undergo fast distribution to lymph nodes and reach steady state after 7 days.” doi:10.1159/000536126 (Source: Cambiaso-Daniel J et al.)
- Negi S, Bala L, Shukla S, Chopra D. “Tattoo inks are toxicological risks to human health: a systematic review.” doi:10.1177/07482337221100870 (Source: Negi S et al.)
- Violi JP, Westerhausen MT, Tasevski B, Kundu P, Donald WA. “Toxic metals and carcinogens in tattoo inks available in Australia.” Journal of Hazardous Materials. doi:10.1016/j.jhazmat.2025.140874 (Source: Violi JP et al.)
- Neale PA, Stalter D, Tang JYM, Escher BI. “Bioanalytical evidence that chemicals in tattoo ink can induce adaptive stress responses.” doi:10.1016/j.jhazmat.2015.04.051 (Source: Neale PA et al.)
- Capucetti A, Falivene J, Pizzichetti C, et al. “Tattoo ink induces inflammation in the draining lymph node and alters the immune response to vaccination.” Proc Natl Acad Sci U S A. 2025;122(48):e2510392122. doi:10.1073/pnas.2510392122 (Source: Capucetti A et al.)
- Reis JM, Cardoso JC, Oliveira A. “Challenges of dermoscopic assessment of basal cell carcinoma on tattooed skin.” JAAD Case Reports. doi:10.1016/j.jdcr.2026.01.058 (Source: Reis JM et al.)
- Lehner K, Santarelli F, Vasold R, et al. “Black tattoos entail substantial uptake of genotoxic polycyclic aromatic hydrocarbons (PAH) in human skin and regional lymph nodes.” PLoS One. doi:10.1371/journal.pone.0092787 (Source: Lehner K et al.)
- Regensburger J, Lehner K, Maisch T, et al. “Tattoo inks contain polycyclic aromatic hydrocarbons that additionally generate deleterious singlet oxygen.” Contact Dermatitis. doi:10.1111/j.1600-0625.2010.01068.x (Source: Regensburger J et al.)