Spitz Nevus (ICD-10: D22) ⚠️
Spitz Nevus (Epithelioid and Spindle-Cell Nevus)
Spitz Nevus (also known as epithelioid and spindle-cell nevus) is a benign skin growth that rises above the skin’s surface. Typically acquired, Spitz nevi are more common in individuals under the age of 20, though about 10% of cases are congenital. Spitz nevi are typically solitary lesions, most often appearing in children and young adults. Spitz nevi are equally common in both men and women.
Predisposing Factors
The exact cause of Spitz nevi is not entirely understood, but there are several predisposing factors that may contribute to the formation of these benign skin lesions. These factors can increase the likelihood of developing Spitz nevi:
- Genetic Factors: A genetic predisposition may contribute to the appearance of Spitz nevi, suggesting a potential hereditary link.
- Ultraviolet Radiation: Exposure to artificial or solar ultraviolet radiation is a known trigger for the development of new nevi, including Spitz nevi.
- Hormonal Changes: Hormonal fluctuations, particularly during puberty or pregnancy, may play a role in the development of Spitz nevi, as these changes can affect the skin and immune system.
Diagnostics
The diagnosis of Spitz nevus is based on a clinical examination, which includes visual inspection and dermatoscopic evaluation. Dermatoscopy allows for a detailed examination of the nevus to identify specific patterns that characterize Spitz nevi. If there is concern about potential malignancy, a biopsy may be performed to confirm the diagnosis and rule out other conditions, such as melanoma.
Symptoms
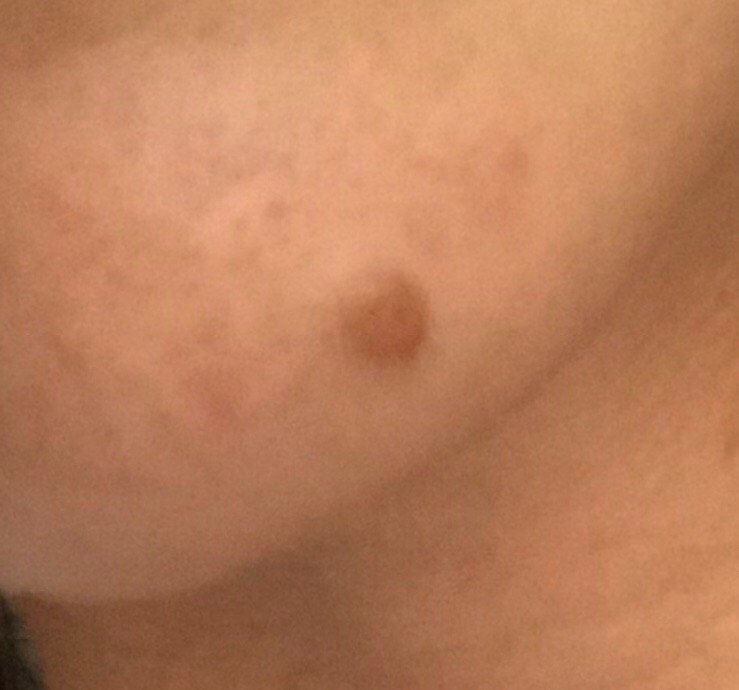
Spitz nevi typically present as hemispherical or slightly flattened lesions that rise above the surface of the skin, most often in a symmetrical shape (oval or round). In some cases, large Spitz nevi can be irregular in shape. The surface of the nevus may be slightly different from the texture of the surrounding skin, either smoother or finely tuberous, giving it a subtle raised appearance. The borders of Spitz nevi are typically clear and even, although larger lesions may have uneven edges.
The color of a Spitz nevus can range from light red (intense flesh-colored) to dark brown, with uniform pigment distribution throughout the lesion. In some cases, there may be a gradual decrease in color intensity from the center to the periphery, or subtle variations of the same color across the nevus. This gradual color change is more typical of larger lesions and is characteristic of verrucous forms of Spitz nevi.
Hair growth is typically absent within the area of a Spitz nevus, which serves as a key distinguishing feature in the differential diagnosis of this type of lesion.
The size of a typical Spitz nevus ranges from 3 mm to 8 mm in diameter. The height above the skin’s surface generally does not exceed 5-7 mm. Larger nevi are rare, and any significant increase in size should be evaluated by a specialist.
On palpation, Spitz nevi are slightly denser than the surrounding skin. Typically, there are no subjective sensations associated with these nevi, but mild itching or tenderness may occasionally be observed in long-standing cases.
Spitz nevi are most commonly found on the face, neck, and limbs, with less frequent occurrences on the body. Their locations typically correspond to areas of the skin that are more susceptible to UV exposure.
Dermatoscopic Description
Dermatoscopy of a Spitz nevus reveals the following characteristic features:
- Star Pattern: A hallmark feature of Spitz nevi, this pattern consists of pigment strips, dots, and/or globules radiating from the center to the periphery.
- Symmetric Blue-White Structure: A symmetric blue-white structure often appears in the center of the nevus, surrounded by pigmented elements such as spots.
- Elasticity and Deformation: Spitz nevi exhibit elasticity, and upon compression, the lesion temporarily becomes paler and smaller.
- Vascular Network: The lesion often shows a diffuse, slightly curved, monomorphic vascular pattern (regular vasculature).
- Diffuse Uniform Staining: The entire formation may be uniformly pigmented under dermatoscopic examination.
Differential Diagnosis
Spitz nevi must be differentiated from other pigmented neoplasms, including:
- Simple nevus
- Papillomatous nevus
- Molluscum contagiosum
- Blue nevus
- Dysplastic nevus
- Basal cell carcinoma
- Melanoma
Risks
Spitz nevi are generally benign, but some lesions can mimic melanoma histologically and require careful evaluation and, in selected cases, excision for histology. Signs of possible malignancy include sudden changes in the appearance of the nevus, such as rapid growth, color change, or development of pain or tenderness — these warrant prompt clinical evaluation.
Malignant transformation of Spitz nevi is rare, but suspicious or changing lesions should be evaluated promptly. However, careful monitoring is essential, especially when there are changes in the lesion’s characteristics.
Tactics
Because Spitz nevi can be difficult to distinguish from melanoma — especially in adults or changing lesions — clinical evaluation is recommended, and excision for histology may be needed in selected cases. This should include annual checks, or more frequent checks in hard-to-see areas with the help of others. If mechanical damage to the nevus occurs, or if there are any noticeable changes, a consultation with a dermatologist or oncologist is necessary.
The healthcare provider will determine whether dynamic monitoring is sufficient or if removal of the nevus is necessary. Nevi that are subject to chronic trauma from clothing, jewelry, or professional activities should be considered for removal to prevent further injury.
For those undergoing dynamic observation, it is useful to photograph the lesion to monitor any changes over time. Patients with multiple nevi should undergo a dermatological examination in the spring and autumn (before and after the sun exposure season). Keeping a map of skin neoplasms can help with monitoring and tracking any changes.
Treatment
The treatment of Spitz nevi is primarily surgical and typically involves excision using either a classic scalpel or a radiofrequency scalpel. A histological examination of the excised tissue is necessary to confirm that the lesion is benign.
Destructive methods such as laser removal or cryodestruction are not recommended for Spitz nevi, as these methods may not allow for proper histological evaluation, and there is a risk of missing potential malignant transformation.
Prevention
Prevention of Spitz nevi and their potential malignancy involves maintaining a careful approach to skin care:
- Limiting exposure to ultraviolet radiation, including avoiding tanning beds and excessive sun exposure.
- Using sunscreen and protective clothing during periods of high sun exposure.
- Avoiding chronic skin trauma that could increase the risk of skin irritation and potential lesion formation.
- Minimizing exposure to ionizing radiation and environmental hazards.
- Maintaining good personal hygiene and staying vigilant for changes in skin health.
Regularly monitoring Spitz nevi, consulting with a healthcare professional if any changes are observed, and removing potentially dangerous lesions when necessary are key to maintaining skin health and minimizing the risk of complications.